

Bimodal Radiotherapy with Active Raster-Scanning Carbon Ion Radiotherapy and Intensity-Modulated Radiotherapy in High-Risk Nasopharyngeal Carcinoma Results in Excellent Local Control
- PMID: 30884910
- PMCID: PMC6468442
- DOI: 10.3390/cancers11030379
Bimodal Radiotherapy with Active Raster-Scanning Carbon Ion Radiotherapy and Intensity-Modulated Radiotherapy in High-Risk Nasopharyngeal Carcinoma Results in Excellent Local Control
Abstract
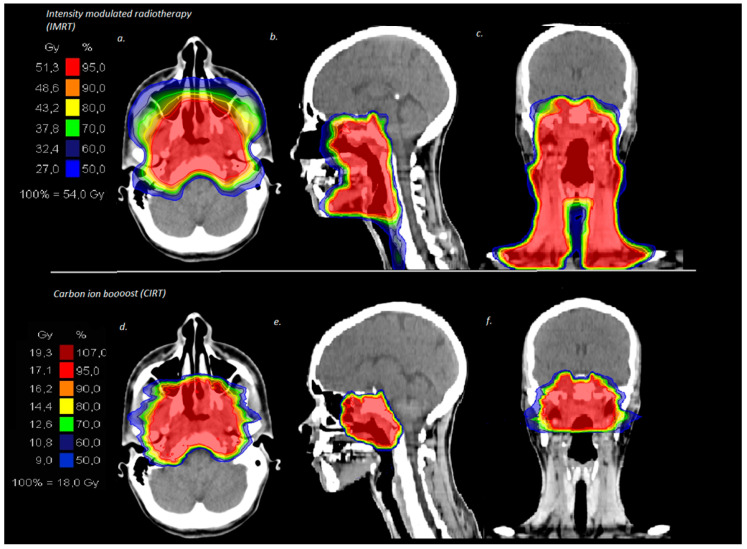
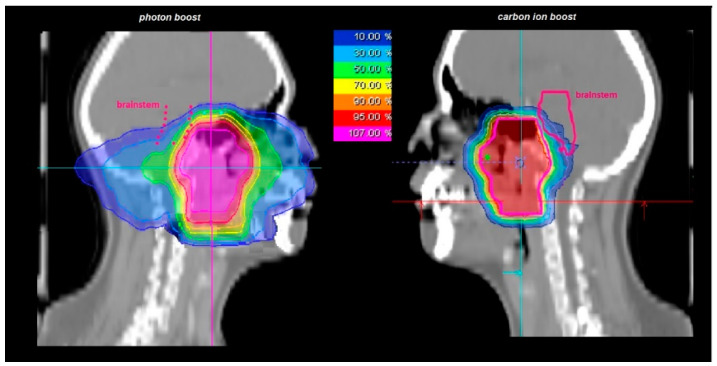
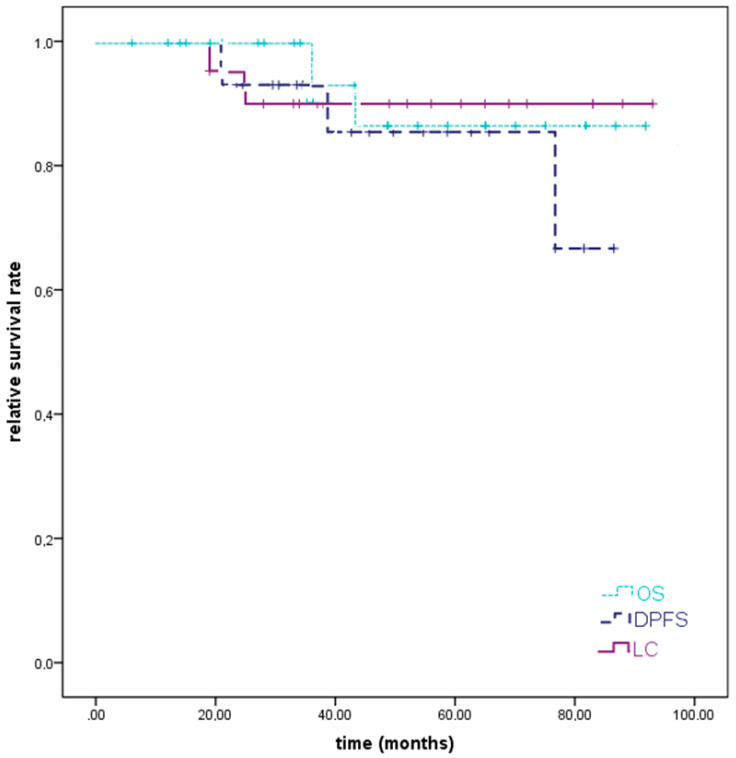
Background: In this analysis, we aimed to present the first results of carbon ion radiotherapy (CIRT), which is known for its conformal dose distribution and increased biological effectiveness in the treatment of high-risk nasopharyngeal carcinoma (NPC). Methods: We retrospectively analyzed twenty-six consecutive patients who had been treated at our center with CIRT for high-risk NPC between 2009 and 2018. Carbon ion (C12) boost was applied in a bimodal setting combined with intensity-modulated radiotherapy (IMRT) base plan. The median cumulative total dose was 74 Gy (RBE), and patients with inoperable (n = 17, 65%) or incompletely resected (n = 7, 27%) tumors were included in the analysis. Overall, 81% received concomitant chemotherapy (n = 21). Results: The median follow-up time was 40 months (range 10⁻97 months) for all patients. At the last follow-up, 92% of the patients were still alive. We could identify excellent tumor response with complete tumor remission (CR) in 60% (n = 15/25), partial tumor remission (PR) in 20% (n = 5/25), and stable disease (SD) in 12% (n = 3/25) of the patients according to the RECIST (Response Evaluation Criteria in Solid Tumors) criteria. Despite unfavorable tumor characteristics, only one patient showed a locally in-field recurrence after 56 months (4%) and another patient a locoregional recurrence in the unilateral cervical lymph nodes after 21 months (4%). The 2-year local control (LC), distant progression-free survival (DPFS), and overall survival (OS) were 95%, 93%, and 100% and the estimated 5-year LC, DPFS, and OS were 90%, 86%, and 86%, respectively. Overall, treatment was tolerated well with 20% acute and 16% chronic grade 3 side effects. No toxicity greater than grade 3 occurred. Conclusion: Bimodal radiotherapy including IMRT and active raster-scanning CIRT for high-risk nasopharyngeal cancer is a safe treatment method resulting in moderate toxicity and excellent local control. A larger patient number and longer follow-up time would be necessary to strengthen the current findings.
Keywords: bimodal radiotherapy; carbon ion radiotherapy; carbon ions; local control; nasopharyngeal cancer; recurrence patterns; survival; toxicity.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Particle beam therapy for nasopharyngeal cancer: A systematic review and meta-analysis.Clin Transl Radiat Oncol. 2022 Aug 23;37:41-56. doi: 10.1016/j.ctro.2022.08.011. eCollection 2022 Nov. Clin Transl Radiat Oncol. 2022. PMID: 36065359 Free PMC article. Review.
-
Results of a combination treatment with intensity modulated radiotherapy and active raster-scanning carbon ion boost for adenoid cystic carcinoma of the minor salivary glands of the nasopharynx.Oral Oncol. 2019 Apr;91:39-46. doi: 10.1016/j.oraloncology.2019.02.019. Epub 2019 Feb 27. Oral Oncol. 2019. PMID: 30926061
-
The impact of age on the outcome of patients treated with radiotherapy for mucoepidermoid carcinoma (MEC) of the salivary glands in the head and neck: A 15-year single-center experience.Oral Oncol. 2019 Oct;97:115-123. doi: 10.1016/j.oraloncology.2019.08.018. Epub 2019 Sep 5. Oral Oncol. 2019. PMID: 31494395
-
Accelerated Hypofractionated Active Raster-Scanned Carbon Ion Radiotherapy (CIRT) for Laryngeal Malignancies: Feasibility and Safety.Cancers (Basel). 2018 Oct 18;10(10):388. doi: 10.3390/cancers10100388. Cancers (Basel). 2018. PMID: 30340397 Free PMC article.
-
The Future of Combining Carbon-Ion Radiotherapy with Immunotherapy: Evidence and Progress in Mouse Models.Int J Part Ther. 2016 Summer;3(1):61-70. doi: 10.14338/IJPT-15-00023.1. Epub 2016 Aug 29. Int J Part Ther. 2016. PMID: 31772976 Free PMC article. Review.
Cited by
-
Particle beam therapy for nasopharyngeal cancer: A systematic review and meta-analysis.Clin Transl Radiat Oncol. 2022 Aug 23;37:41-56. doi: 10.1016/j.ctro.2022.08.011. eCollection 2022 Nov. Clin Transl Radiat Oncol. 2022. PMID: 36065359 Free PMC article. Review.
-
Flourish of Proton and Carbon Ion Radiotherapy in China.Front Oncol. 2022 Feb 14;12:819905. doi: 10.3389/fonc.2022.819905. eCollection 2022. Front Oncol. 2022. PMID: 35237518 Free PMC article. Review.
-
Clustered DNA Double-Strand Breaks: Biological Effects and Relevance to Cancer Radiotherapy.Genes (Basel). 2020 Jan 15;11(1):99. doi: 10.3390/genes11010099. Genes (Basel). 2020. PMID: 31952359 Free PMC article. Review.
-
Current Radiotherapy Considerations for Nasopharyngeal Carcinoma.Cancers (Basel). 2022 Nov 24;14(23):5773. doi: 10.3390/cancers14235773. Cancers (Basel). 2022. PMID: 36497254 Free PMC article. Review.
-
The Particle Radiobiology of Multipotent Mesenchymal Stromal Cells: A Key to Mitigating Radiation-Induced Tissue Toxicities in Cancer Treatment and Beyond?Front Oncol. 2021 Apr 12;11:616831. doi: 10.3389/fonc.2021.616831. eCollection 2021. Front Oncol. 2021. PMID: 33912447 Free PMC article. Review.
References
-
- Barnes L., Eveson J.W., Reichert P., Sidransky D. World Health Organization Classification of Tumors. IARC Press; Lyon, France: 2005. Pathology and genetics of head and neck tumors.
-
- Pan J.J., Ng W.T., Zong J.F., Chan L.L., O’Sullivan B., Lin S.J., Sze H.C., Chen Y.B., Choi H.C., Guo Q.J., et al. Proposal for the 8th edition of the AJCC/UICC staging system for nasopharyngeal cancer in the era of intensity-modulated radiotherapy. Cancer. 2016;122:546–558. doi: 10.1002/cncr.29795. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
