

Quest for the best endoscopic imaging modality for computer-assisted colonic polyp staging
- PMID: 30886503
- PMCID: PMC6421240
- DOI: 10.3748/wjg.v25.i10.1197
Quest for the best endoscopic imaging modality for computer-assisted colonic polyp staging
Abstract
Background: It was shown in previous studies that high definition endoscopy, high magnification endoscopy and image enhancement technologies, such as chromoendoscopy and digital chromoendoscopy [narrow-band imaging (NBI), i-Scan] facilitate the detection and classification of colonic polyps during endoscopic sessions. However, there are no comprehensive studies so far that analyze which endoscopic imaging modalities facilitate the automated classification of colonic polyps. In this work, we investigate the impact of endoscopic imaging modalities on the results of computer-assisted diagnosis systems for colonic polyp staging.
Aim: To assess which endoscopic imaging modalities are best suited for the computer-assisted staging of colonic polyps.
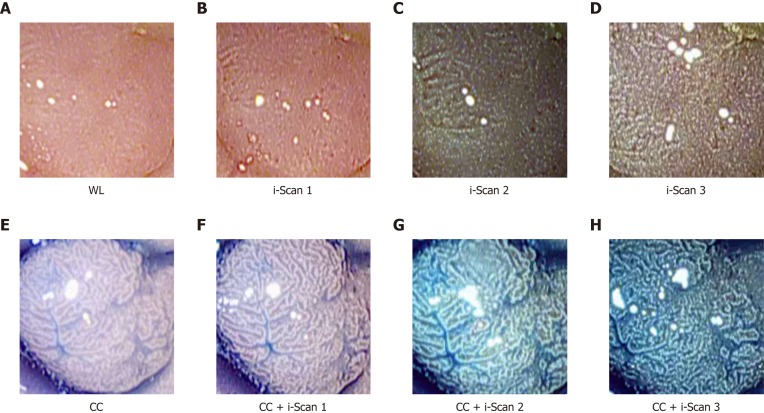
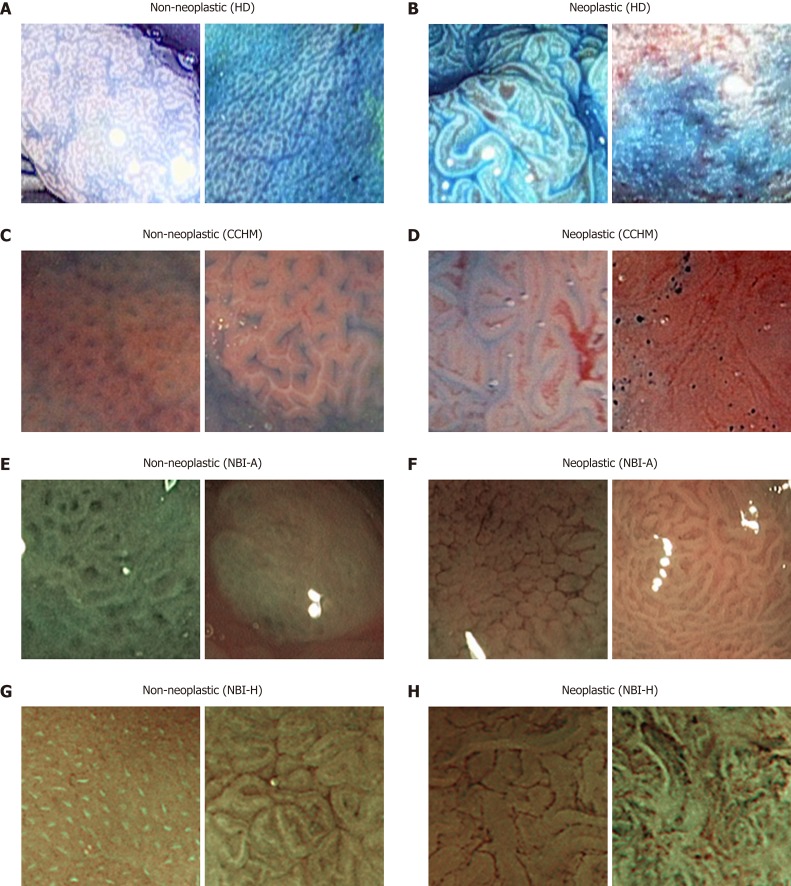
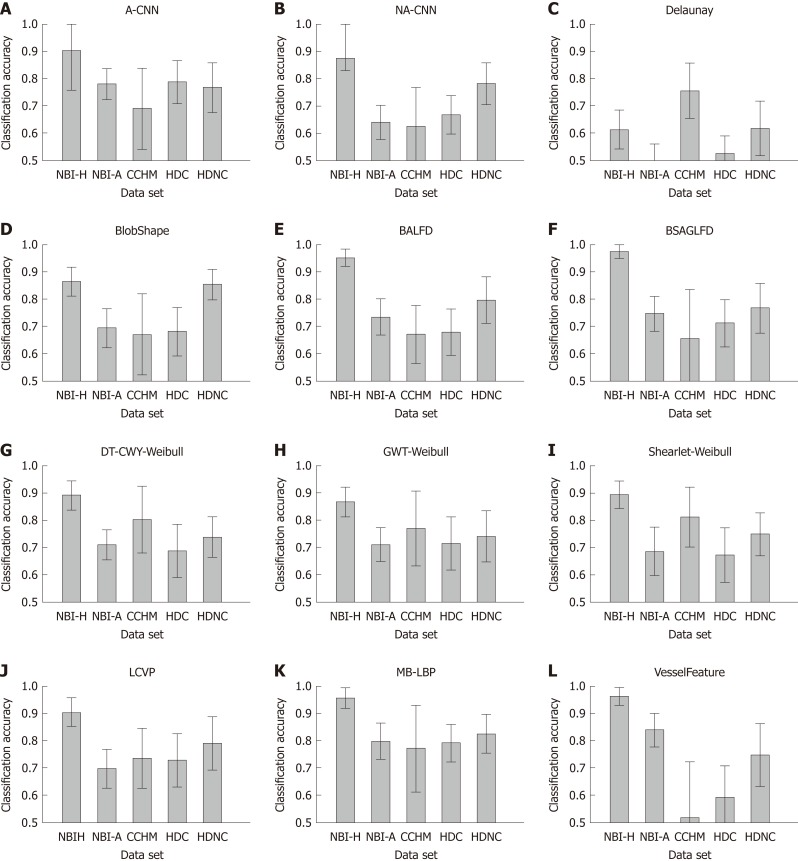
Methods: In our experiments, we apply twelve state-of-the-art feature extraction methods for the classification of colonic polyps to five endoscopic image databases of colonic lesions. For this purpose, we employ a specifically designed experimental setup to avoid biases in the outcomes caused by differing numbers of images per image database. The image databases were obtained using different imaging modalities. Two databases were obtained by high-definition endoscopy in combination with i-Scan technology (one with chromoendoscopy and one without chromoendoscopy). Three databases were obtained by high-magnification endoscopy (two databases using narrow band imaging and one using chromoendoscopy). The lesions are categorized into non-neoplastic and neoplastic according to the histological diagnosis.
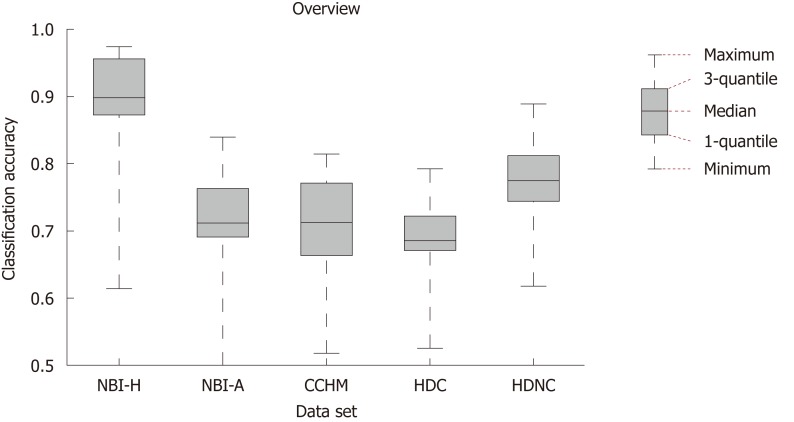
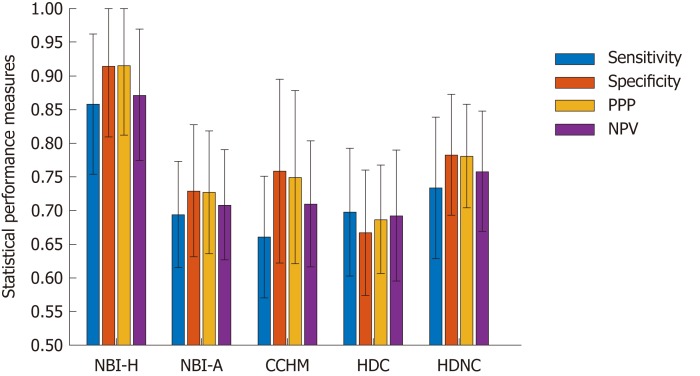
Results: Generally, it is feature-dependent which imaging modalities achieve high results and which do not. For the high-definition image databases, we achieved overall classification rates of up to 79.2% with chromoendoscopy and 88.9% without chromoendoscopy. In the case of the database obtained by high-magnification chromoendoscopy, the classification rates were up to 81.4%. For the combination of high-magnification endoscopy with NBI, results of up to 97.4% for one database and up to 84% for the other were achieved. Non-neoplastic lesions were classified more accurately in general than non-neoplastic lesions. It was shown that the image recording conditions highly affect the performance of automated diagnosis systems and partly contribute to a stronger effect on the staging results than the used imaging modality.
Conclusion: Chromoendoscopy has a negative impact on the results of the methods. NBI is better suited than chromoendoscopy. High-definition and high-magnification endoscopy are equally suited.
Keywords: Automated diagnosis system; Chromoendoscopy; Colonic polyps; Endoscopy; Image enhancement technologies; Imaging modalities; Narrow-band imaging.
Conflict of interest statement
Conflict-of-interest statement: There are no conflicts of interest.
Figures
Similar articles
-
Training of polyp staging systems using mixed imaging modalities.Comput Biol Med. 2018 Nov 1;102:251-259. doi: 10.1016/j.compbiomed.2018.05.003. Epub 2018 May 4. Comput Biol Med. 2018. PMID: 29773226
-
Value of magnifying chromoendoscopy and narrow band imaging (NBI) in classifying colorectal polyps: a prospective controlled study.Endoscopy. 2007 Dec;39(12):1092-6. doi: 10.1055/s-2007-966781. Endoscopy. 2007. PMID: 18072061 Clinical Trial.
-
Virtual chromoendoscopy for the real-time assessment of colorectal polyps in vivo: a systematic review and economic evaluation.Health Technol Assess. 2017 Dec;21(79):1-308. doi: 10.3310/hta21790. Health Technol Assess. 2017. PMID: 29271339 Free PMC article.
-
A prospective comparative study of narrow-band imaging, chromoendoscopy, and conventional colonoscopy in the diagnosis of colorectal neoplasia.Gut. 2007 Mar;56(3):373-9. doi: 10.1136/gut.2006.099614. Epub 2006 Sep 27. Gut. 2007. PMID: 17005766 Free PMC article.
-
Additional chromoendoscopy for colorectal lesions initially diagnosed with low confidence by magnifying narrow-band imaging: Can it improve diagnostic accuracy?Dig Endosc. 2018 Apr;30 Suppl 1:45-50. doi: 10.1111/den.13055. Dig Endosc. 2018. PMID: 29658652 Review.
Cited by
-
Artificial Intelligence Enhances Studies on Inflammatory Bowel Disease.Front Bioeng Biotechnol. 2021 Jul 8;9:635764. doi: 10.3389/fbioe.2021.635764. eCollection 2021. Front Bioeng Biotechnol. 2021. PMID: 34307315 Free PMC article. Review.
References
-
- Berr F, Oyama T, Ponchon T, Yahagi N. Early Neoplasias of the Gastrointestinal Tract: Endoscopic Diagnosis and Therapeutic Decisions. Boston: Springer; 2014.
-
- Rex DK, Kahi C, O'Brien M, Levin TR, Pohl H, Rastogi A, Burgart L, Imperiale T, Ladabaum U, Cohen J, Lieberman DA. The American Society for Gastrointestinal Endoscopy PIVI (Preservation and Incorporation of Valuable Endoscopic Innovations) on real-time endoscopic assessment of the histology of diminutive colorectal polyps. Gastrointest Endosc. 2011;73:419–422. - PubMed
-
- Patel SG, Schoenfeld P, Kim HM, Ward EK, Bansal A, Kim Y, Hosford L, Myers A, Foster S, Craft J, Shopinski S, Wilson RH, Ahnen DJ, Rastogi A, Wani S. Real-Time Characterization of Diminutive Colorectal Polyp Histology Using Narrow-Band Imaging: Implications for the Resect and Discard Strategy. Gastroenterology. 2016;150:406–418. - PMC - PubMed
-
- ASGE Technology Committee. Manfredi MA, Abu Dayyeh BK, Bhat YM, Chauhan SS, Gottlieb KT, Hwang JH, Komanduri S, Konda V, Lo SK, Maple JT, Murad FM, Siddiqui UD, Wallace MB, Banerjee S. Electronic chromoendoscopy. Gastrointest Endosc. 2015;81:249–261. - PubMed
-
- Hoffman A, Kagel C, Goetz M, Tresch A, Mudter J, Biesterfeld S, Galle PR, Neurath MF, Kiesslich R. Recognition and characterization of small colonic neoplasia with high-definition colonoscopy using i-Scan is as precise as chromoendoscopy. Dig Liver Dis. 2010;42:45–50. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
