

Endoloop ligation after endoscopic mucosal resection using a transparent cap: A novel method to treat small rectal carcinoid tumors
- PMID: 30886508
- PMCID: PMC6421235
- DOI: 10.3748/wjg.v25.i10.1259
Endoloop ligation after endoscopic mucosal resection using a transparent cap: A novel method to treat small rectal carcinoid tumors
Abstract
Background: Local endoscopic resection is an effective method for the treatment of small rectal carcinoid tumors, but remnant tumor at the margin after resection remains to be an issue.
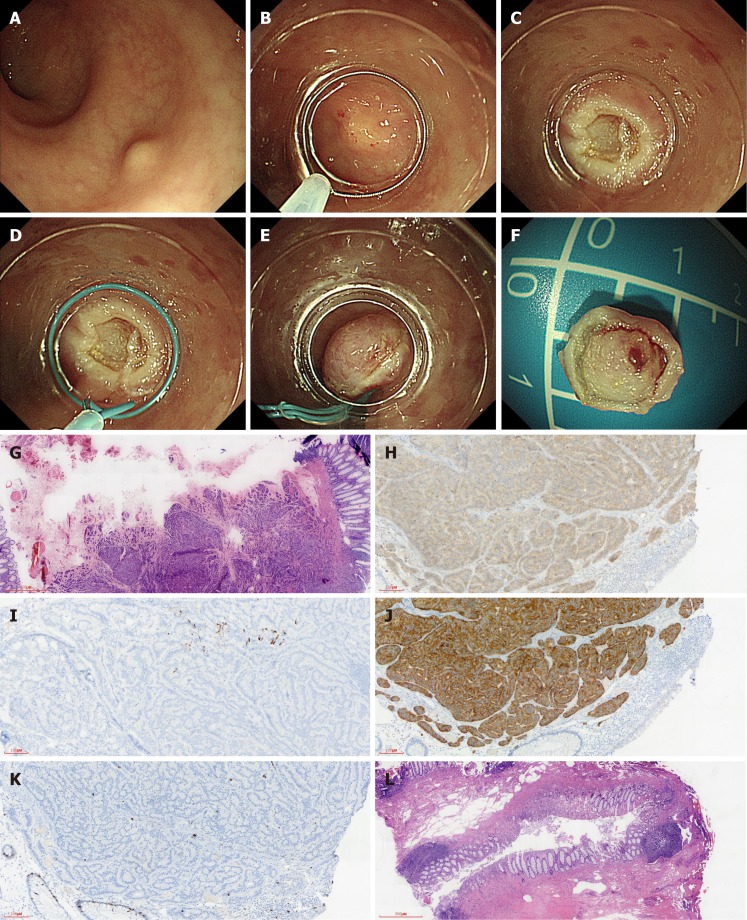
Aim: To evaluate the efficacy and safety of resection of small rectal carcinoid tumors by endoloop ligation after cap-endoscopic mucosal resection (LC-EMR) using a transparent cap.
Methods: Thirty-four patients with rectal carcinoid tumors of less than 10 mm in diameter were treated by LC-EMR (n = 22) or endoscopic submucosal dissection (ESD) (n = 12) between January 2016 and December 2017. Demographic data, complete resection rates, pathologically complete resection rates, operation duration, and postoperative complications were collected. All cases were followed for 6 to 30 mo.
Results: A total of 22 LC-EMR cases and 12 ESD cases were enrolled. The average age was 48.18 ± 12.31 and 46.17 ± 12.57 years old, and the tumor size was 7.23 ± 1.63 mm and 7.50 ± 1.38 mm, respectively, for the LC-EMR and ESD groups. Resection time in the ESD group was longer than that in the LC-EMR group (15.67 ± 2.15 min vs 5.91 ± 0.87 min; P < 0.001). All lesions were completely resected at one time. No perforation or delayed bleeding was observed in either group. Pathologically complete resection (P-CR) rate was 86.36% (19/22) and 91.67% (11/12) in the LC-EMR and ESD groups (P = 0.646), respectively. Two of the three cases with a positive margin in the LC-EMR group received transanal endoscopic microsurgery (TEM) and tumor cells were not identified in the postoperative specimens. The other case with a positive margin chose follow-up without further operation. One case with remnant tumor after ESD received further local ligation treatment. Neither local recurrence nor lymph node metastasis was found during the follow-up period.
Conclusion: LC-EMR appears to be an efficient and simple method for the treatment of small rectal carcinoid tumors, which can effectively avoid margin remnant tumors.
Keywords: Endoscopic mucosal resection; Endoscopic submucosal dissection; Ligation; Rectal carcinoid.
Conflict of interest statement
Conflict-of-interest statement: The authors declare no conflicts of interest.
Figures
Similar articles
-
The clinical outcomes and risk factors associated with incomplete endoscopic resection of rectal carcinoid tumor.Surg Endosc. 2017 Dec;31(12):5006-5011. doi: 10.1007/s00464-017-5497-x. Epub 2017 Sep 21. Surg Endosc. 2017. PMID: 28936630
-
Treatment outcomes of endoscopic resection for rectal carcinoid tumors: an analysis of the resectability and long-term results from 46 consecutive cases.Scand J Gastroenterol. 2016 Dec;51(12):1489-1494. doi: 10.1080/00365521.2016.1216591. Epub 2016 Aug 9. Scand J Gastroenterol. 2016. PMID: 27687741
-
Comparison of endoscopic resection therapies for rectal carcinoid tumor: endoscopic submucosal dissection versus endoscopic mucosal resection using band ligation.J Clin Gastroenterol. 2013 May-Jun;47(5):432-6. doi: 10.1097/MCG.0b013e31826faf2b. J Clin Gastroenterol. 2013. PMID: 23188074
-
Endoscopic submucosal dissection versus endoscopic mucosal resection for rectal carcinoid tumor. A meta-analysis and meta-regression with single-arm analysis.J Dig Dis. 2021 Oct;22(10):562-571. doi: 10.1111/1751-2980.13048. J Dig Dis. 2021. PMID: 34472210 Review.
-
Endoscopic submucosal dissection (ESD) versus transanal endoscopic microsurgery (TEM) for treatment of rectal tumors: a comparative systematic review and meta-analysis.Surg Endosc. 2020 Apr;34(4):1688-1695. doi: 10.1007/s00464-019-06945-1. Epub 2019 Jul 10. Surg Endosc. 2020. PMID: 31292744
Cited by
-
A new endoscopic submucosal resection -ligation technique for gastric tumors.Gastroenterol Hepatol Bed Bench. 2020 Winter;13(Suppl1):S149-S153. Gastroenterol Hepatol Bed Bench. 2020. PMID: 33585018 Free PMC article.
-
Endoscopic full thickness resection vs. transanal endoscopic microsurgery for local treatment of rectal neuroendocrine tumors - a retrospective analysis.Int J Colorectal Dis. 2021 May;36(5):971-976. doi: 10.1007/s00384-020-03800-x. Epub 2020 Nov 19. Int J Colorectal Dis. 2021. PMID: 33215239 Free PMC article.
-
Application of in vivo traction-assisted resection of proximal colon lesions: a case series (with video).Surg Endosc. 2022 Nov;36(11):8231-8236. doi: 10.1007/s00464-022-09266-y. Epub 2022 May 5. Surg Endosc. 2022. PMID: 35511341
-
Risk factors for regional lymph node metastasis in rectal neuroendocrine tumors: a population-based study.Front Med (Lausanne). 2024 Sep 4;11:1383047. doi: 10.3389/fmed.2024.1383047. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39296902 Free PMC article.
-
Efficacy of endoscopic mucosal resection versus endoscopic submucosal dissection for rectal neuroendocrine tumors ≤10mm: a systematic review and meta-analysis.Ann Saudi Med. 2023 May-Jun;43(3):179-195. doi: 10.5144/0256-4947.2023.179. Epub 2023 Jun 1. Ann Saudi Med. 2023. PMID: 37270677 Free PMC article.
References
-
- Koura AN, Giacco GG, Curley SA, Skibber JM, Feig BW, Ellis LM. Carcinoid tumors of the rectum: effect of size, histopathology, and surgical treatment on metastasis free survival. Cancer. 1997;79:1294–1298. - PubMed
-
- Shields CJ, Tiret E, Winter DC International Rectal Carcinoid Study Group. Carcinoid tumors of the rectum: a multi-institutional international collaboration. Ann Surg. 2010;252:750–755. - PubMed
-
- Yoshikane H, Goto H, Niwa Y, Matsui M, Ohashi S, Suzuki T, Hamajima E, Hayakawa T. Endoscopic resection of small duodenal carcinoid tumors with strip biopsy technique. Gastrointest Endosc. 1998;47:466–470. - PubMed
-
- Lee DS, Jeon SW, Park SY, Jung MK, Cho CM, Tak WY, Kweon YO, Kim SK. The feasibility of endoscopic submucosal dissection for rectal carcinoid tumors: comparison with endoscopic mucosal resection. Endoscopy. 2010;42:647–651. - PubMed
-
- Zhang D, Lin Q, Shi R, Wang L, Yao J, Tian Y. Ligation-assisted endoscopic submucosal resection with apical mucosal incision to treat gastric subepithelial tumors originating from the muscularis propria. Endoscopy. 2018;50:1180–1185. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
