

Evaluating the impact of the ICNET® clinical decision support system for antimicrobial stewardship
- PMID: 30886704
- PMCID: PMC6404285
- DOI: 10.1186/s13756-019-0496-4
Evaluating the impact of the ICNET® clinical decision support system for antimicrobial stewardship
Abstract
Background: Antimicrobial resistance (AMR) is an ecological and economic crisis and stewardship of available antimicrobials is required. Electronic prescribing, where available, enables auditing of practice, yet in order to be efficient and effective in addressing inappropriate antimicrobial prescribing, better use of current and new technological interventions is needed. This retrospective observational evaluation looked at the impact of a commercial clinical decision support system (CDSS) on the workflow of an established antimicrobial stewardship (AMS) team.
Material/methods: Clinical, workflow, and pharmaceutical data from 3 months post implementation of CDSS were collated, and compared to the same 3 month periods in preceding years. The evaluation considered total interventions made, the types of intervention made, impact of said interventions, and time spent executing interventions. All antimicrobial data were adjusted for total daily defined doses (DDD) of intravenous antimicrobials.
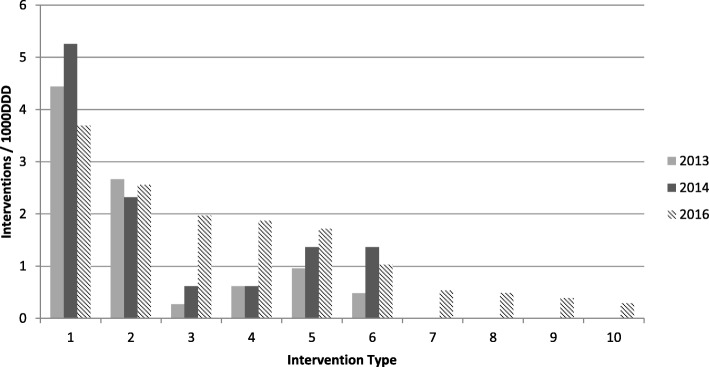
Results: Productivity: In the 3 month evaluation period (Jun-Aug 2016) a total of 264 case reviews resulting in 298 AMS interventions were made. Compared to preceding years where 138 and 169 interventions were made (2013 and 2014 respectively). In 2013 49% of interventions were stopping medication and 30% change of therapy based on cultures and sensitivities compared to 25 and 17% in 2016. In contrast to previous years', the CDSS instead enabled a greater number of dose/drug optimisation (13%), escalation of antimicrobials (12%) and intravenous (IV) to oral switch (11%) interventions.Patient Identification: Despite increased patient numbers post-CDSS, on average 46 min per day was spent compiling a patient list for review, compared to 59 min in 2014. The use of CDSS facilitated 15 interventions/1000DDD, compared to pre-intervention (9.4/1000DDD in 2013; 11.5/1000DDD in 2014).
Conclusions: Initial evaluation of the impact of this CDSS on AMS at the organisation has demonstrated effectiveness in terms of case finding, AMS team productivity, and workflow auditing. More importantly, patient infection management has been optimised with a shift in the emphasis of AMS interventions. It has contributed to the success of the healthcare provider achieving nationally set remunerated AMS targets.
Keywords: Antimicrobial resistance; Antimicrobial stewardship; Clinical decision support system; eHealth; mHealth.
Conflict of interest statement
Approval was gained for this project as a service evaluation from the Joint Research Compliance Office, Chelsea & Westminster Hospital Campus, Imperial College London (ref: CAPP 1327, July 2015). Data was collected as routine and no patient level data was used.No patient identifiable data necessitating consent was used in this study.LSPM has consulted for bioMerieux (2013), DNAelectronics (2015), Dairy Crest (2017–2018), received speaker fees from Profile Pharma (2018) and Pfizer (2018), received research grants from the National Institute for Health Research (2013–2018) and Leo Pharma (2016), and received educational support from Eumedica (2016–2017). NM has consulted for Beyer (2016) and received educational support from Eumedica (2016) and Baxter (2017). SH has received educational support from Baxter (2017). All other authors have no conflicts of interest to declare.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- World Health Organisation: Global Action Plan on Antimicrobial Resistance. 2015. http://www.who.int/antimicrobial-resistance/publications/global-action-p.... Accessed 23 June 2018.
-
- Public Health England: English surveillance programme for antimicrobial utilisation and resistance. 2014. https://assets.publishing.service.gov.uk/government/uploads/system/uploa... Accessed 23 June 2018.
-
- Public Health England: Antibiotic Guardian. 2014. http://antibioticguardian.com/ . Accessed 22 May 2018.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
