

Giant cell arteritis: pathogenic mechanisms and new potential therapeutic targets
- PMID: 30886946
- PMCID: PMC6383596
- DOI: 10.1186/s41927-017-0004-5
Giant cell arteritis: pathogenic mechanisms and new potential therapeutic targets
Abstract
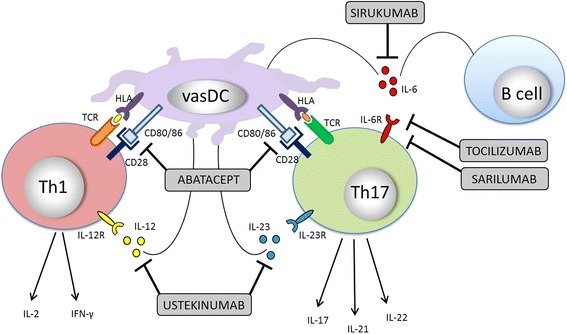
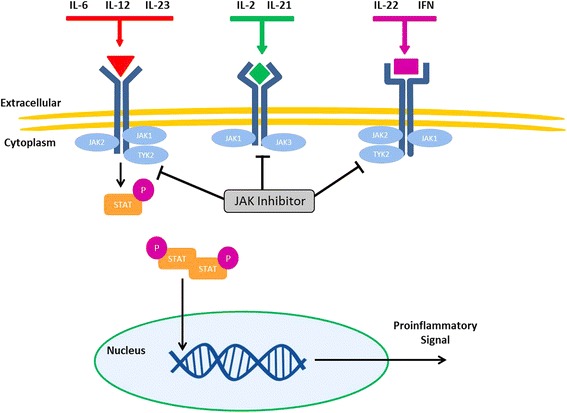
Giant cell arteritis (GCA) is the most common idiopathic systemic vasculitis in persons aged 50 years or greater. Treatment options for GCA, to-date, have been limited and have consisted primarily of glucocorticoids. Significant advances in the understanding of the genetic and cellular mechanisms in GCA are leading to identification of potential pathogenic targets. The recent success of interleukin-6 blockade in the treatment of GCA has opened the landscape to targeted biologic therapy. T cells, particularly T helper 1 and T helper 17 cell lineages have been identified as key inflammatory cells in both active and chronic vascular inflammatory lesions. Therapeutic agents, including abatacept and ustekinumab, which can impede both vasculitogenic cell lines are of particular interest. Inhibition of signalling pathways, including the janus kinase-signal tranducers and activation of transcription (JAK-STAT) and Notch pathways are evolving options. Tocilizumab has shown clear benefit in both newly diagnosed and relapsing patients with GCA and approval of this medication for treatment of GCA has led to rapid incorporation into treatment regimens. More information is required to understand the long-term outcomes of tocilizumab and other investigational targeted therapeutics in the treatment of GCA.
Keywords: Biologics; Giant cell arteritis; Pathogenesis; Therapeutics; Vasculitis.
Conflict of interest statement
Not applicable.Not applicable.The authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Combe B, Sany J, Le Quellec A, Clot J, Eliaou JF: Distribution of HLA-DRB1 alleles of patients with polymyalgia rheumatica and giant cell arteritis in a Mediterranean population. J Rheumatol. 1998;25(1):94-98. - PubMed
-
- Dababneh A, Gonzalez-Gay MA, Garcia-Porrua C, Hajeer A, Thomson W, Ollier W. Giant cell arteritis and polymyalgia rheumatica can be differentiated by distinct patterns of HLA class II association. J Rheumatol. 1998;25(11):2140–2145. - PubMed
-
- Jacobsen S, Baslund B, Madsen HO, Tvede N, Svejgaard A, Garred P. Mannose-binding lectin variant alleles and HLA-DR4 alleles are associated with giant cell arteritis. J Rheumatol. 2002;29(10):2148–2153. - PubMed
-
- Martinez-Taboda VM, Bartolome MJ, Lopez-Hoyos M, Blanco R, Mata C, Calvo J, Corrales A, Rodriguez-Valverde V. HLA-DRB1 allele distribution in polymyalgia rheumatica and giant cell arteritis: influence on clinical subgroups and prognosis. Semin Arthritis Rheum. 2004;34(1):454–464. doi: 10.1016/j.semarthrit.2003.12.001. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
