

The extra-articular impacts of rheumatoid arthritis: moving towards holistic care
- PMID: 30886982
- PMCID: PMC6390577
- DOI: 10.1186/s41927-018-0039-2
The extra-articular impacts of rheumatoid arthritis: moving towards holistic care
Abstract
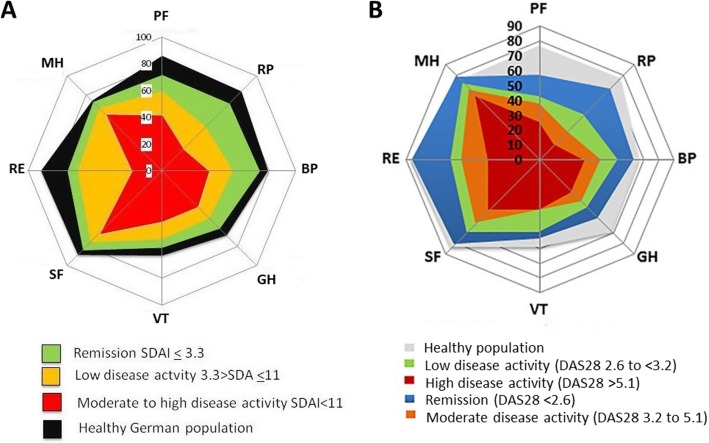
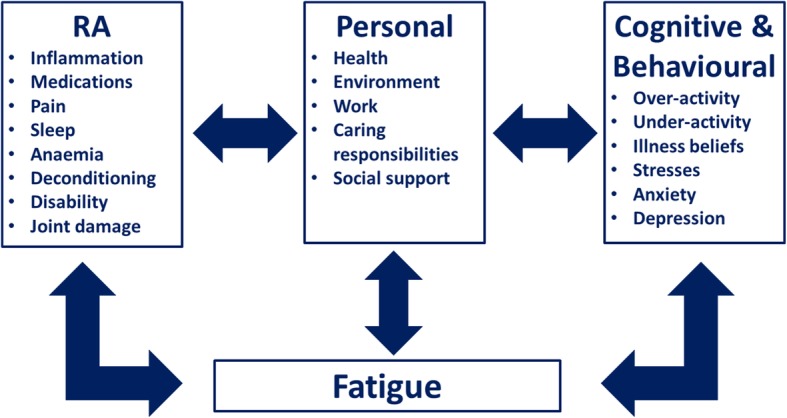
Although treat-to-target has revolutionised the outcomes of patients with rheumatoid arthritis (RA) there is emerging evidence that attaining the target of remission is insufficient to normalise patients' quality of life, and ameliorate the extra-articular impacts of RA. RA has a broad range of effects on patient's lives, with four key "extra-articular" impacts being pain, depression and anxiety, fatigue and rheumatoid cachexia. All of these are seen frequently; for example, studies have reported that 1 in 4 patients with RA have high-levels of fatigue. Commonly used drug treatments (including simple analgesics, non-steroidal anti-inflammatory drugs and anti-depressants) have, at most, only modest benefits and often cause adverse events. Psychological strategies and dynamic and aerobic exercise all reduce issues like pain and fatigue, although their effects are also only modest. The aetiologies of these extra-articular impacts are multifactorial, but share overlapping components. Consequently, patients are likely to benefit from management strategies that extend beyond the assessment and treatment of synovitis, and incorporate more broad-based, or "holistic", assessments of the extra-articular impacts of RA and their management, including non-pharmacological approaches. Innovative digital technologies (including tablet and smartphone "apps" that directly interface with hospital systems) are increasingly available that can directly capture patient-reported outcomes during and between clinic visits, and include them within electronic patient records. These are likely to play an important future role in delivering such approaches.
Keywords: Cachexia; Fatigue; Mental health; Pain; Rheumatoid arthritis.
Conflict of interest statement
Not applicable.Not applicable.The authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Drossaers-Bakker KW, de Buck M, van Zeben D, Zwinderman AH, Breedveld FC, Hazes JM. Long-term course and outcome of functional capacity in rheumatoid arthritis: the effect of disease activity and radiologic damage over time. Arthritis Rheum. 1999;42(9):1854–1860. doi: 10.1002/1529-0131(199909)42:9<1854::AID-ANR9>3.0.CO;2-F. - DOI - PubMed
-
- Welsing PM, van Gestel AM, Swinkels HL, Kiemeney LA, van Riel PL. The relationship between disease activity, joint destruction, and functional capacity over the course of rheumatoid arthritis. Arthritis Rheum. 2001;44(9):2009–2017. doi: 10.1002/1529-0131(200109)44:9<2009::AID-ART349>3.0.CO;2-L. - DOI - PubMed
-
- Klarenbeek NB, Koevoets R, van der Heijde DMFM, Gerards AH, Ten Wolde S, Kerstens PJSM, et al. Association with joint damage and physical functioning of nine composite indices and the 2011 ACR/EULAR remission criteria in rheumatoid arthritis. Ann Rheum Dis. 2011;70(10):1815–1821. doi: 10.1136/ard.2010.149260. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
