

Real world long-term impact of intensive treatment on disease activity, disability and health-related quality of life in rheumatoid arthritis
- PMID: 30886994
- PMCID: PMC6390620
- DOI: 10.1186/s41927-019-0054-y
Real world long-term impact of intensive treatment on disease activity, disability and health-related quality of life in rheumatoid arthritis
Abstract
Background: The emphasis on treating rheumatoid arthritis (RA) intensively reduces disease activity but its impact in routine care is uncertain. We evaluated temporal changes in disease activities and outcomes in a 10-year prospective observational cohort study of patients in routine care at one unit.
Methods: The Guy's and St Thomas' RA cohort was established in 2005. It involved most RA patients managed in this hospital. Clinical diagnoses of RA were made by rheumatologists. Patients were seen regularly in routine care. Each visit included measurement of disease activity scores for 28 joints (DAS28), health assessment questionnaire scores (HAQ) and EuroQol scores. Patients received intensive treatments targeting DAS28 remission.
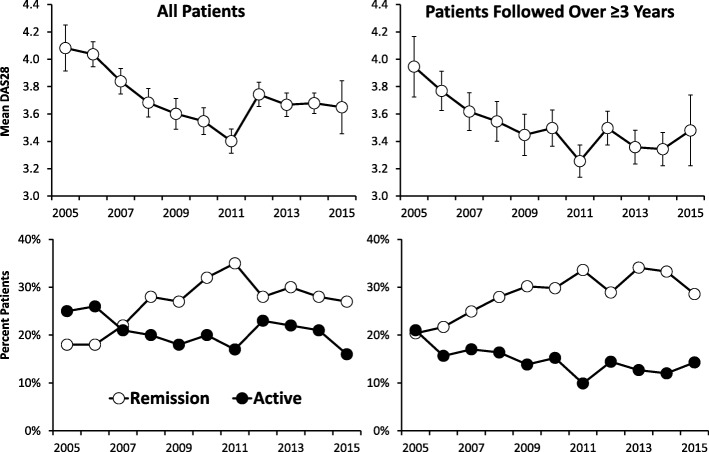
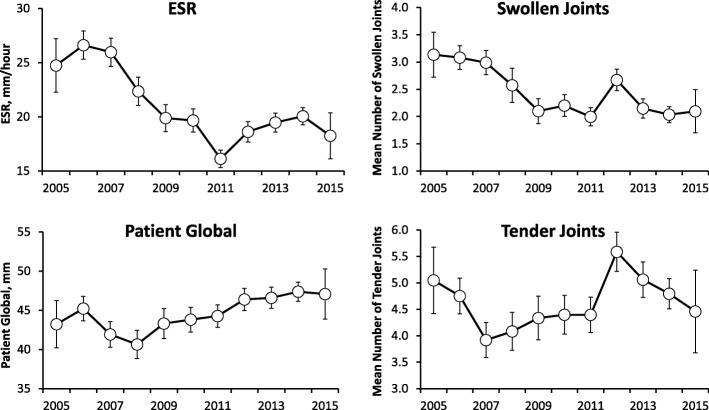
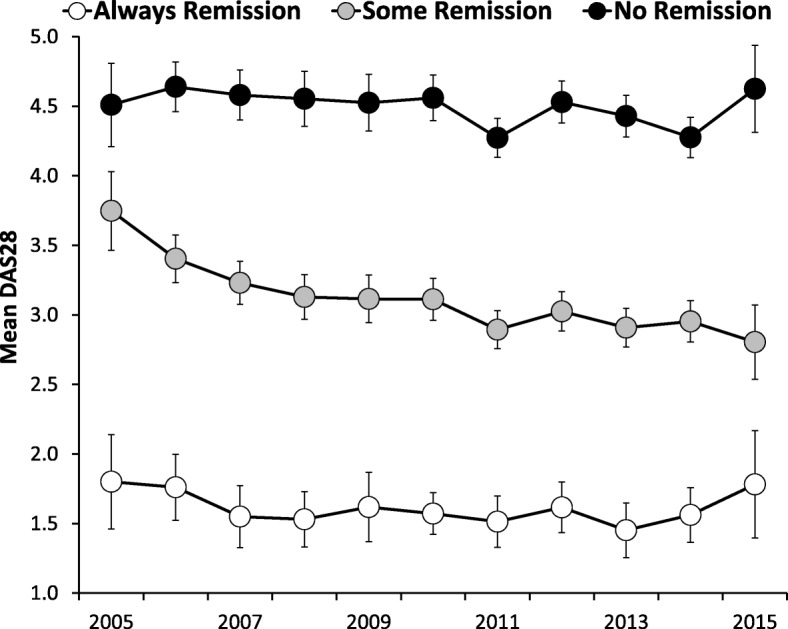
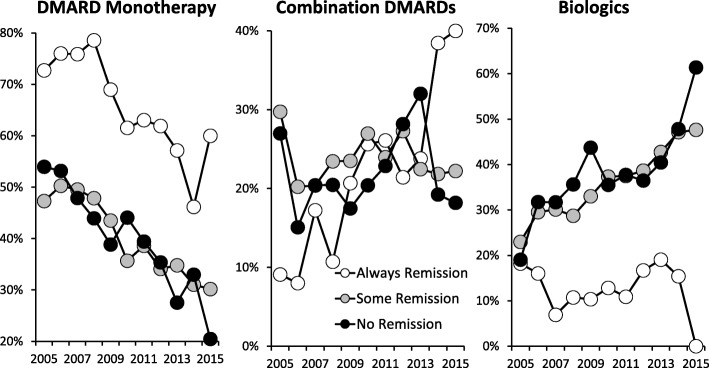
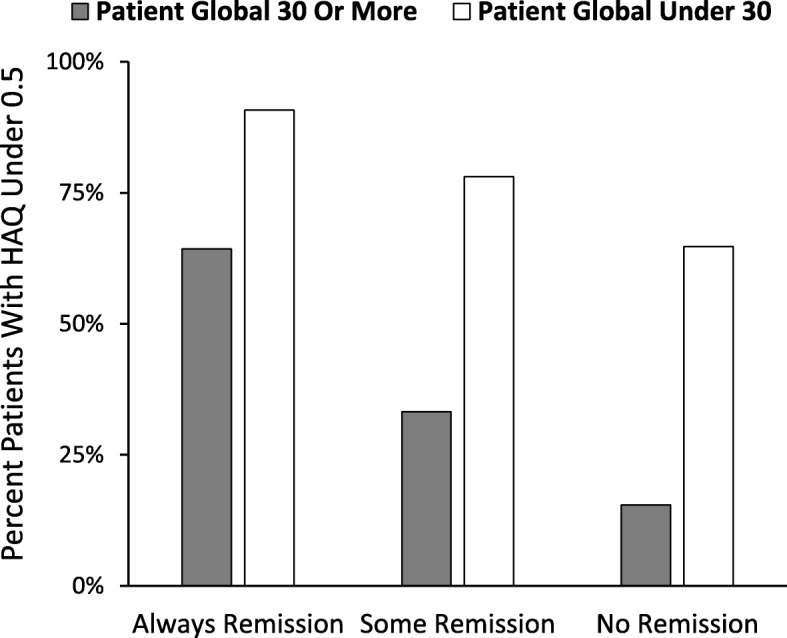
Results: In 1693 RA patients mean DAS28 scores fell from 2005 to 15 by 11% from 4.08 (95% CI: 3.91, 4.25) in 2005 to 3.64 (3.34, 3.78); these falls were highly significant (p < 0.001). DAS28 components: swollen joint counts fell by 32% and ESR by 24%; in contrast tender joint counts and patient global assessments showed minimal or no reductions. The reduction in DAS28 scores was predominantly between 2005 and 2010, with no falls from 2011 onwards. Associated with falls in mean DAS28s, patients achieving remission increased (18% in 2005; 27% in 2015) and the number with active disease (DAS28 > 5.1) decreased (25% in 2005; 16% in 2015). In 752 patients seen at least annually for 3 years, persisting remission (68 patients) and intermittent remission (376 patients) were associated with less disability and better health related quality of life. Over time biologic use increased, but they were used infrequently in patients in persistent remission.
Conclusions: Over 10 years an intensive management strategy in a routine practice setting increased combination DMARD and biologic use: disease activity levels declined; this association is in keeping with a causal relationship. Patients who achieved remission, even transiently, had better functional outcomes than patients never achieving remission.
Keywords: Intensive treatment; Rheumatoid arthritis; Temporal RA change.
Conflict of interest statement
Ethics approval for analysis of routine clinical data was obtained from the Health Research Authority (IRAS project ID: 209418). The need for consent was waived due to the use of of previously collected, de-identified data, and complies with the Helsinki Declaration.Not applicable.The authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Rheumatoid arthritis in adults: management NICE guidelines 2009 (updated 2015) CG79. https://www.nice.org.uk/Guidance/CG79. Accessed 1 June 2018.
-
- Singh JA, Saag KG, Bridges SL, et al. 2015 American College of Rheumatology Guideline for the treatment of rheumatoid arthritis. Arthritis Rheumatol. 2016;68:1–26. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
