

Low PI-RADS assessment category excludes extraprostatic extension (≥pT3a) of prostate cancer: a histology-validated study including 301 operated patients
- PMID: 30887199
- PMCID: PMC6719329
- DOI: 10.1007/s00330-019-06092-0
Low PI-RADS assessment category excludes extraprostatic extension (≥pT3a) of prostate cancer: a histology-validated study including 301 operated patients
Abstract
Objectives: To evaluate whether low PI-RADS v2 assessment categories are effective at excluding extraprostatic extension (EPE) of prostate cancer (≥pT3a PCa).
Methods: The local institutional ethics committee approved this retrospective analysis of 301 consecutive PCa patients. Patients were classified as low- or intermediate/high-risk based on clinical parameters and underwent pre-surgical multiparametric magnetic resonance imaging. A PI-RADS v2 assessment category and ESUR EPE score were assigned for each lesion by two readers working in consensus. Histopathologic analysis of the whole-mount radical prostatectomy specimen was the reference standard. Univariate and multivariate analyses were performed to evaluate the association of PI-RADS v2 assessment category with final histology ≥pT3a PCa.
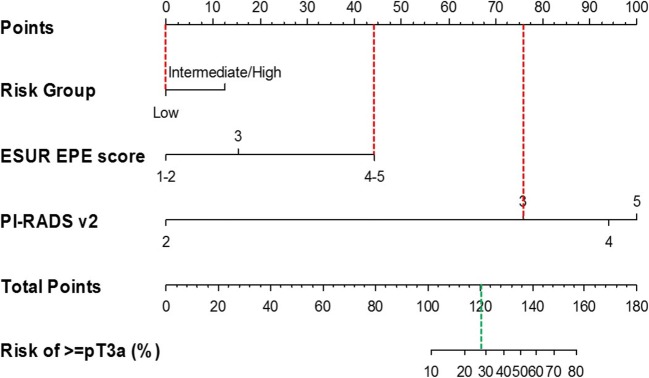
Results: For a PI-RADS v2 assessment category threshold of 3, the overall performance for ruling out (sensitivity, negative predictive value, negative likelihood ratio) ≥pT3a PCa was 99%/98%/0.04 and was similar in both the low-risk (96%/97%/0.12; N = 137) and the intermediate/high-risk groups (100%/100%/0.0; N = 164). In univariate analysis, all clinical and tumor characteristics except age were significantly associated with ≥pT3a PCa. In multivariate analysis, PI-RADS v2 assessment categories ≤ 3 had a protective effect relative to categories 4 and 5. The inclusion of ESUR EPE score improved the AUC of ≥pT3a PCa prediction (from 0.73 to 0.86, p = 0.04 in the overall cohort). The impact of PI-RADS v2 assessment category is reflected in a nomogram derived on the basis of our cohort.
Conclusions: In our cohort, low PI-RADS v2 assessment categories of 3 or less confidently ruled out the presence of ≥pT3a PCa irrespective of clinical risk group.
Key points: • Our analysis of 301 mp-MRI and RARP specimens showed that the addition of PI-RADS v2 assessment categories to clinical parameters improves the exclusion of ≥pT3a (extraprostatic) prostate cancer. • PI-RADS v2 assessment categories of 1 to 3 are useful for excluding ≥pT3a prostate cancer with a NPV of 98%; such patients can be considered as candidates for less invasive approaches. • The ability to exclude ≥pT3a prostate cancer may improve confidence in choosing nerve-sparing surgery or in avoiding pelvic nodal dissections, and similarly for patients undergoing radiotherapy, in adopting short-course adjuvant hormonal therapy or foregoing prophylactic nodal irradiation.
Keywords: Magnetic resonance imaging; Nomogram; Prostate cancer.
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Figures
Similar articles
-
PI-RADS v2 and periprostatic fat measured on multiparametric magnetic resonance imaging can predict upgrading in radical prostatectomy pathology amongst patients with biopsy Gleason score 3 + 3 prostate cancer.Scand J Urol. 2018 Oct-Dec;52(5-6):333-339. doi: 10.1080/21681805.2018.1545799. Scand J Urol. 2018. PMID: 30895901
-
Effect of observation size and apparent diffusion coefficient (ADC) value in PI-RADS v2.1 assessment category 4 and 5 observations compared to adverse pathological outcomes.Eur Radiol. 2020 Aug;30(8):4251-4261. doi: 10.1007/s00330-020-06725-9. Epub 2020 Mar 24. Eur Radiol. 2020. PMID: 32211965
-
Prostate Cancer: The European Society of Urogenital Radiology Prostate Imaging Reporting and Data System Criteria for Predicting Extraprostatic Extension by Using 3-T Multiparametric MR Imaging.Radiology. 2015 Aug;276(2):479-89. doi: 10.1148/radiol.15141412. Epub 2015 Apr 3. Radiology. 2015. PMID: 25848900
-
Extraprostatic extension in prostate cancer: primer for radiologists.Abdom Radiol (NY). 2020 Dec;45(12):4040-4051. doi: 10.1007/s00261-020-02555-x. Abdom Radiol (NY). 2020. PMID: 32390076 Review.
-
A meta-analysis of use of Prostate Imaging Reporting and Data System Version 2 (PI-RADS V2) with multiparametric MR imaging for the detection of prostate cancer.Eur Radiol. 2017 Dec;27(12):5204-5214. doi: 10.1007/s00330-017-4843-7. Epub 2017 Jun 27. Eur Radiol. 2017. PMID: 28656462 Review.
Cited by
-
Imaging features of the PI-RADS for predicting extraprostatic extension of prostate cancer: systematic review and meta-analysis.Insights Imaging. 2023 May 8;14(1):77. doi: 10.1186/s13244-023-01422-9. Insights Imaging. 2023. PMID: 37156971 Free PMC article.
-
Can we predict pathology without surgery? Weighing the added value of multiparametric MRI and whole prostate radiomics in integrative machine learning models.Eur Radiol. 2024 Oct;34(10):6241-6253. doi: 10.1007/s00330-024-10699-3. Epub 2024 Mar 20. Eur Radiol. 2024. PMID: 38507053
-
Long-term follow-up results of multiparametric prostate MRI and the prognostic value of PI-RADS: a single-center retrospective cohort study.Diagn Interv Radiol. 2024 May 13;30(3):139-151. doi: 10.4274/dir.2023.232414. Epub 2023 Sep 19. Diagn Interv Radiol. 2024. PMID: 37724756 Free PMC article.
-
Periprostatic Adipose Tissue: A New Perspective for Diagnosing and Treating Prostate Cancer.J Cancer. 2024 Jan 1;15(1):204-217. doi: 10.7150/jca.89750. eCollection 2024. J Cancer. 2024. PMID: 38164282 Free PMC article. Review.
-
The Role of Magnetic Resonance Imaging and Positron Emission Tomography/Computed Tomography in the Primary Staging of Newly Diagnosed Prostate Cancer: A Systematic Review of the Literature.Eur Urol Oncol. 2021 Jun;4(3):370-395. doi: 10.1016/j.euo.2020.11.002. Epub 2020 Dec 4. Eur Urol Oncol. 2021. PMID: 33272865 Free PMC article.
References
-
- National Comprehensive Cancer Network (NCCN) (2012) NCCN clinical practice guidelines in oncology: prostate cancer. https://www.nccn.org/professionals/physician_gls/default.aspx#site. Accessed 7 July 2018
-
- de Rooij M, Hamoen EH, Fütterer JJ, Barentsz JO, Rovers MM (2014) Accuracy of multiparametric MRI for prostate cancer detection: a metaanalysis. AJR Am J Roentgenol 202:343–351 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
