

Two-year patient-related outcome measures (PROM) of primary ventral and incisional hernia repair using a novel three-dimensional composite polyester monofilament mesh: the SymCHro registry study
- PMID: 30887379
- PMCID: PMC6661060
- DOI: 10.1007/s10029-019-01924-w
Two-year patient-related outcome measures (PROM) of primary ventral and incisional hernia repair using a novel three-dimensional composite polyester monofilament mesh: the SymCHro registry study
Abstract
Purpose: This study examined patient-related outcome measures (PROMs) after repair of ventral primary or incisional hernias using Symbotex™ composite mesh (SCM), a novel three-dimensional collagen-coated monofilament polyester textile.
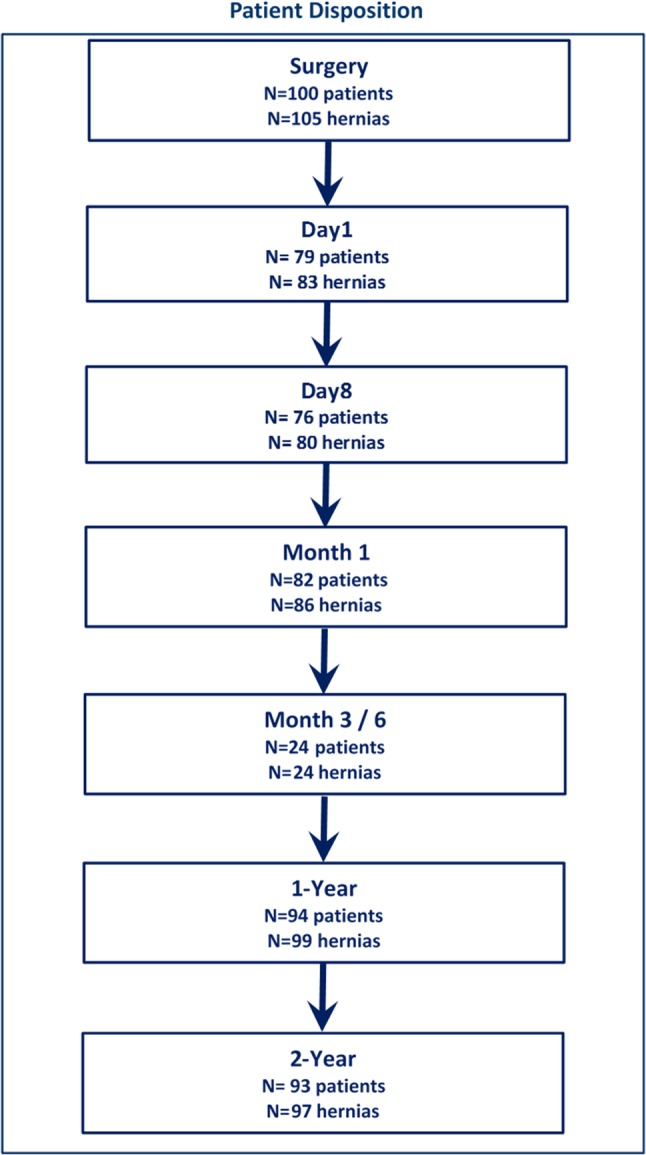
Methods: Pre-operative, peri-operative, and post-operative data were obtained from the French "Club Hernie" registry with 12- and 24-month follow-up.
Results: One-hundred consecutive patients (mean age 62.0 ± 13.7; 51% female) underwent repair of 105 hernias: primary (39/105, 37.1%, defect area 5.2 ± 5.6 cm2) and incisional (66/105, 62.9%, 31.9 ± 38.7.8 cm2). The mean BMI was 29.7 (± 5.6 kg/m2). American Society of Anesthesiologists classifications were I 39.4%, II 37.4% and III 23.2%. 75% had risk factors for healing and/or dissection. Of 38 primary repairs, 37 were completed laparoscopically (combined approach n = 1), and of 62 incisional hernia repairs, 40 were completed laparoscopically, and 20 by open repair (combined approach n = 2). Laparoscopic was quicker than open repair (36.2 ± 23.5 min vs. 67.4 ± 25.8, p < 0001). Before surgery, 86.3% of hernias were reported to cause discomfort/pain or dysesthesia. At 24 months (93 of 100 patients), 91 (97.8%) reported no lump and 81 (87.1%) no pain or discomfort. Of 91 patients, 86 (94.5%) rated their repair "good" or "excellent." There were nine non-serious, surgeon-detected adverse events (ileus, n = 3; seroma, n = 6) and one hernia recurrence (6-12 months).
Conclusions: Compared to baseline, open and laparoscopic surgery improved PROMs 24 months after primary and incisional hernia repair. Minimal complications and recurrence support the long-term efficacy of SCM.
Keywords: Abdominal hernia; Hernia repair; Incisional hernia; Laparoscopy; Surgical mesh; Ventral hernia.
Conflict of interest statement
JG declares conflict of interest not directly related to the submitted work (x). ML declares conflict of interest not directly related to the submitted work (x). CB declares conflict of interest not directly related to the submitted work (x). OC declares conflict of interest not directly related to the submitted work (x). AD declares conflict of interest not directly related to the submitted work (x). FJ declares no conflict of interest. HK declares conflict of interest not directly related to the submitted work (x). CZ declares conflict of interest not directly related to the submitted work (x). J.F. Gillion: President of Club-Hernie and organizer of the annual Mesh Congress. He has received expert honorarium and/or non-financial support from Medtronic, Bard Davol, Cousin Biotech, MSD and Gore. M. Lepere: Non-financial support from Medtronic. C. Barrat: Consultant for Medtronic. Grants and/or fees from Bard Davol, Johnson & Johnson, MSD and Gore. O. Cas: Research funding from Medtronic. A. Dabrowski: Non-financial support from Medtronic. F. Jurczak: No conflict of interest. H. Khalil: Non-financial support from Medtronic. C. Zaranis: Relations with Bard DAvol, Cousin Biotech, MSD and Gore. RE, outside the submitted work.
Figures
References
-
- Kroese LF, Kleinrensink GJ, Lange JF, Gillion JF, Hernia C. External validation of the European Hernia Society Classification for postoperative complications after incisional hernia repair: a cohort study of 2191 patients. J Am Coll Surg. 2018;226(3):223–229 e1. doi: 10.1016/j.jamcollsurg.2017.11.018. - DOI - PubMed
-
- Sauerland S, Walgenbach M, Habermalz B, Seiler CM, Miserez M. Laparoscopic versus open surgical techniques for ventral or incisional hernia repair. Cochrane Database Syst Rev. 2011;3:Cd007781. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
