

Concise Review: Boosting T-Cell Reconstitution Following Allogeneic Transplantation-Current Concepts and Future Perspectives
- PMID: 30887712
- PMCID: PMC6591542
- DOI: 10.1002/sctm.18-0248
Concise Review: Boosting T-Cell Reconstitution Following Allogeneic Transplantation-Current Concepts and Future Perspectives
Abstract
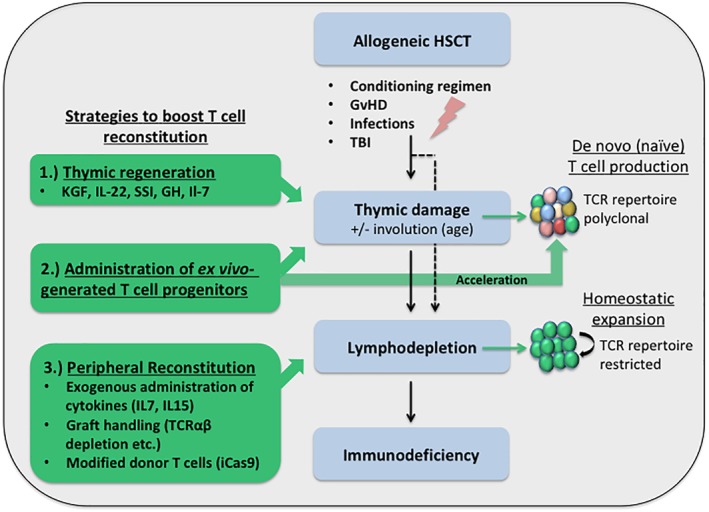
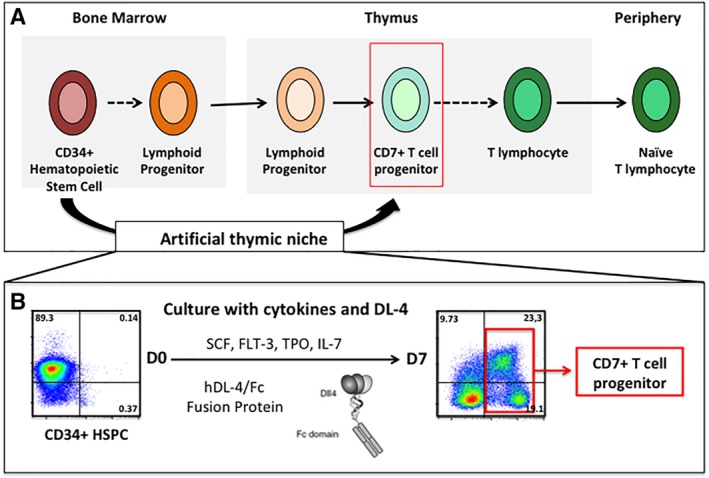
Allogeneic hematopoietic stem cell transplantation (HSCT) is the treatment of choice for a large number of malignant and nonmalignant (inherited) diseases of the hematopoietic system. Nevertheless, non-HLA identical transplantations are complicated by a severe T-cell immunodeficiency associated with a high rate of infection, relapse and graft-versus-host disease. Initial recovery of T-cell immunity following HSCT relies on peripheral expansion of memory T cells mostly driven by cytokines. The reconstitution of a diverse, self-tolerant, and naive T-cell repertoire, however, may take up to 2 years and crucially relies on the interaction of T-cell progenitors with the host thymic epithelium, which may be altered by GvHD, age or transplant-related toxicities. In this review, we summarize current concepts to stimulate reconstitution of a peripheral and polyclonal T-cell compartment following allogeneic transplantation such as graft manipulation (i.e., T-cell depletion), transfusion of ex vivo manipulated donor T cells or the exogenous administration of cytokines and growth factors to stimulate host-thymopoiesis with emphasis on approaches which have led to clinical trials. Particular attention will be given to the development of cellular therapies such as the ex vivo generation of T-cell precursors to fasten generation of a polyclonal and functional host-derived T-cell repertoire. Having been tested so far only in preclinical mouse models, clinical studies are now on the way to validate the efficacy of such T-cell progenitors in enhancing immune reconstitution following HSCT in various clinical settings. Stem Cells Translational Medicine 2019;00:1-8.
Keywords: Cellular therapy; Hematologic malignancies; Hematopoietic stem cell transplantation; Immune reconstitution; Immunodeficiency; T-cell; Thymus.
© 2019 The Authors. STEM CELLS TRANSLATIONAL MEDICINE published by Wiley Periodicals, Inc. on behalf of AlphaMed Press.
Conflict of interest statement
The authors indicated no potential conflicts of interest.
Figures
Similar articles
-
Thymus and immune reconstitution after allogeneic hematopoietic stem cell transplantation in humans: never say never again.Tissue Antigens. 2012 Feb;79(2):83-9. doi: 10.1111/j.1399-0039.2011.01820.x. Tissue Antigens. 2012. PMID: 22220718 Review.
-
Graft Engineering and Adoptive Immunotherapy: New Approaches to Promote Immune Tolerance After Hematopoietic Stem Cell Transplantation.Front Immunol. 2019 Jul 10;10:1342. doi: 10.3389/fimmu.2019.01342. eCollection 2019. Front Immunol. 2019. PMID: 31354695 Free PMC article. Review.
-
Alloreactivity as therapeutic principle in the treatment of hematologic malignancies. Studies of clinical and immunologic aspects of allogeneic hematopoietic cell transplantation with nonmyeloablative conditioning.Dan Med Bull. 2007 May;54(2):112-39. Dan Med Bull. 2007. PMID: 17521527 Review.
-
T-Cell Progenitors As A New Immunotherapy to Bypass Hurdles of Allogeneic Hematopoietic Stem Cell Transplantation.Front Immunol. 2022 Jul 7;13:956919. doi: 10.3389/fimmu.2022.956919. eCollection 2022. Front Immunol. 2022. PMID: 35874778 Free PMC article. Review.
-
Ex vivo generated human T-lymphoid progenitors as a tool to accelerate immune reconstitution after partially HLA compatible hematopoietic stem cell transplantation or after gene therapy.Bone Marrow Transplant. 2019 Aug;54(Suppl 2):749-755. doi: 10.1038/s41409-019-0599-9. Bone Marrow Transplant. 2019. PMID: 31431705 Review.
Cited by
-
Co‑transplantation of tonsil‑derived mesenchymal stromal cells in bone marrow transplantation promotes thymus regeneration and T cell diversity following cytotoxic conditioning.Int J Mol Med. 2020 Sep;46(3):1166-1174. doi: 10.3892/ijmm.2020.4657. Epub 2020 Jun 24. Int J Mol Med. 2020. PMID: 32582998 Free PMC article.
-
Vaccinations in Pediatric Hematology and Oncology: Biologic Basis, Clinical Applications, and Perspectives.Vaccines (Basel). 2025 Apr 10;13(4):397. doi: 10.3390/vaccines13040397. Vaccines (Basel). 2025. PMID: 40333279 Free PMC article. Review.
-
A Notch/IL-21 signaling axis primes bone marrow T cell progenitor expansion.JCI Insight. 2022 May 9;7(9):e157015. doi: 10.1172/jci.insight.157015. JCI Insight. 2022. PMID: 35349492 Free PMC article.
-
Lower Absolute Lymphocyte Count Before Conditioning Predicts High Relapse Risk in Patients After Haploidentical Peripheral Blood Stem Cell Transplantation With Low Dose Anti-Thymocyte Globulin/Post-Transplant Cyclophosphamide for GvHD Prophylaxis.Cell Transplant. 2022 Jan-Dec;31:9636897221079739. doi: 10.1177/09636897221079739. Cell Transplant. 2022. PMID: 35225024 Free PMC article.
-
Synthesis of an Anti-CD7 Recombinant Immunotoxin Based on PE24 in CHO and E. coli Cell-Free Systems.Int J Mol Sci. 2022 Nov 8;23(22):13697. doi: 10.3390/ijms232213697. Int J Mol Sci. 2022. PMID: 36430170 Free PMC article.
References
-
- Bacigalupo A, Dominietto A, Ghiso A et al. Unmanipulated haploidentical bone marrow transplantation and post‐transplant cyclophosphamide for hematologic malignanices following a myeloablative conditioning: An update. Bone Marrow Transplant 2015;50:S37–S39. - PubMed
-
- Busca A, Locatelli F, Flonta SE et al. In vivo T‐cell depletion with pretransplant low‐dose antithymocyte globulin is associated with reduced transplant‐related mortality and improved clinical outcome in patients receiving allogeneic hematopoietic stem cell transplantation from unrelated and partially matched related donors. Am J Hematol 2011;86:214–217. - PubMed
-
- Sengsayadeth S, Savani BN, Blaise D et al. Haploidentical transplantation: Selecting optimal conditioning regimen and stem cell source. Semin Hematol 2016;53:111–114. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
