

PCR-reverse dot blot human papillomavirus genotyping as a primary screening test for cervical cancer in a hospital-based cohort
- PMID: 30887754
- PMCID: PMC6424850
- DOI: 10.3802/jgo.2019.30.e29
PCR-reverse dot blot human papillomavirus genotyping as a primary screening test for cervical cancer in a hospital-based cohort
Abstract
Objective: To evaluate the polymerase chain reaction (PCR)-reverse-dot-blot (RDB) human papillomavirus (HPV) genotyping test as a feasible assay for the cervical cancer primary screening.
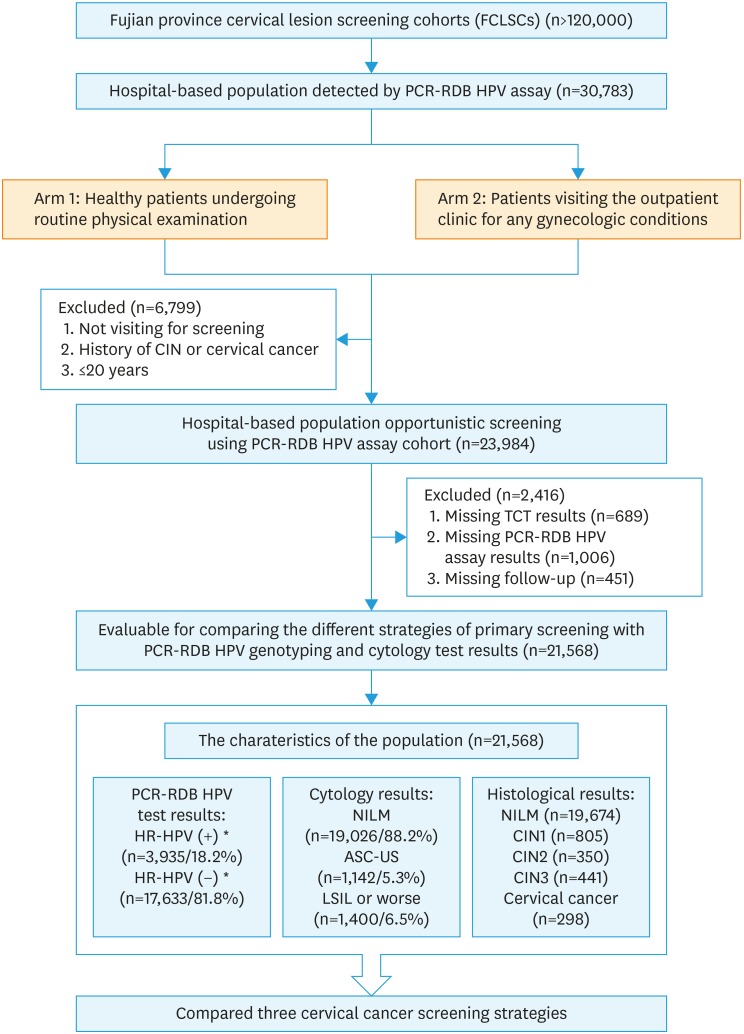
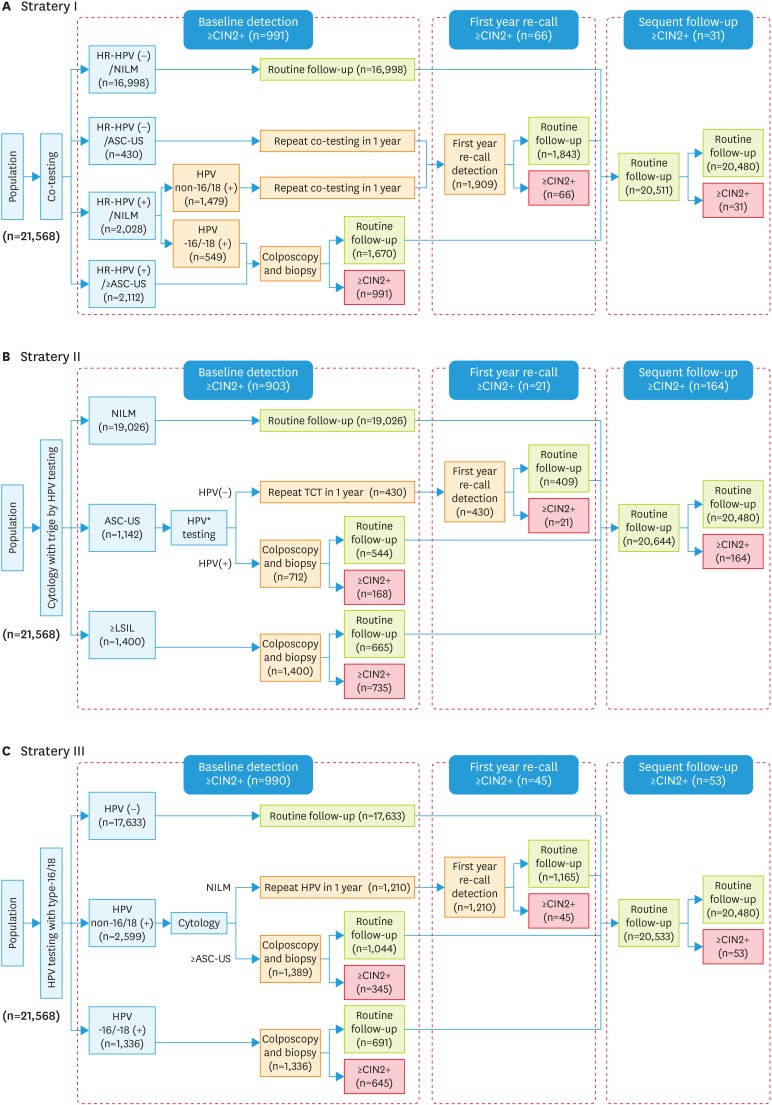
Methods: In a hospital-based cohort, a total of 21,568 women were voluntarily enrolled from March 2009 to November 2016 for evaluating the 3 current cervical cancer screening strategies: co-test, cytology primary and high-risk HPV (HR-HPV) primary by using PCR-RDB HPV genotyping and liquid-based cytology (thinprep cytologic test [TCT]). Women with HR-HPV infection and/or abnormal cytology were referred for colposcopy, and the biopsy or conization was performed according to the American Society for Colposcopy and Cervical Pathology (ASCCP) guidelines.
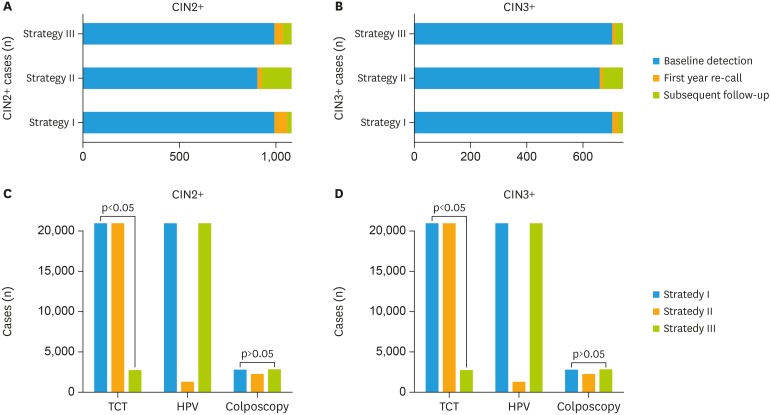
Results: Overall, 18.20% (3,935/21,568) of the women were detected as HR-HPV-positive, 5.04% (1,088/21,568) were diagnosed with cervical intraepithelial neoplasia 2 or higher (CIN2+), and 3.43% (739/21,568) with CIN3+. The cumulative incidence rates for CIN2+/CIN3+ in patients with HPV-16/18-positive were 48.28%/37.20%, while they were 0.86%/0.38%, 0.30%/0.15% and 0.18%/0.09% in cytology-negative, HR-HPV-negative and co-test-negative population, respectively. Using CIN2+ and CIN3+ as the observed endpoints, the sensitivity and negative predictive value (NPV) of HR-HPV genotyping as a primary screening tool were 90.99%/99.49% and 91.57%/99.80%. Moreover, using HR-HPV genotyping primary screening could detect the same more CIN2+/CIN3+ cases in baseline-detection as co-testing (990/700 vs. 991/701) and far more than cytology primary screening (903/656, p<0.05). It also achieved the lowest misdiagnosis rate (8.01%/5.02%). Although HPV genotyping primary screening required an increased number of colposcopies (2.75/3.89 per CIN2+/CIN3+ case), it yielded an acceptable rate.
Conclusions: The PCR-RDB HPV genotyping test is a cost-effective and beneficial cervical cancer primary screening for hospital-based opportunistic screening.
Keywords: Cancer Screening; Cervical Cancer; Cytology; Genotype; Papillomaviridae.
Copyright © 2019. Asian Society of Gynecologic Oncology, Korean Society of Gynecologic Oncology.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Clinical validation of the PCR-reverse dot blot human papillomavirus genotyping test in cervical lesions from Chinese women in the Fujian province: a hospital-based population study.J Gynecol Oncol. 2017 Sep;28(5):e50. doi: 10.3802/jgo.2017.28.e50. Epub 2017 Apr 25. J Gynecol Oncol. 2017. PMID: 28657218 Free PMC article.
-
The clinical effectiveness and cost-effectiveness of primary human papillomavirus cervical screening in England: extended follow-up of the ARTISTIC randomised trial cohort through three screening rounds.Health Technol Assess. 2014 Apr;18(23):1-196. doi: 10.3310/hta18230. Health Technol Assess. 2014. PMID: 24762804 Free PMC article. Clinical Trial.
-
Performance of carcinogenic human papillomavirus (HPV) testing and HPV16 or HPV18 genotyping for cervical cancer screening of women aged 25 years and older: a subanalysis of the ATHENA study.Lancet Oncol. 2011 Sep;12(9):880-90. doi: 10.1016/S1470-2045(11)70188-7. Epub 2011 Aug 22. Lancet Oncol. 2011. PMID: 21865084 Clinical Trial.
-
Accuracy of human papillomavirus testing on self-collected versus clinician-collected samples: a meta-analysis.Lancet Oncol. 2014 Feb;15(2):172-83. doi: 10.1016/S1470-2045(13)70570-9. Epub 2014 Jan 14. Lancet Oncol. 2014. PMID: 24433684 Review.
-
Triage of HPV positive women in cervical cancer screening.J Clin Virol. 2016 Mar;76 Suppl 1(Suppl 1):S49-S55. doi: 10.1016/j.jcv.2015.11.015. Epub 2015 Nov 28. J Clin Virol. 2016. PMID: 26643050 Free PMC article. Review.
Cited by
-
Detection of Five Types of HPV Genotypes Causing Anogenital Warts (Condyloma Acuminatum) Using PCR-Tm Analysis Technology.Front Microbiol. 2022 May 17;13:857410. doi: 10.3389/fmicb.2022.857410. eCollection 2022. Front Microbiol. 2022. PMID: 35655998 Free PMC article.
-
Platelet-to-Lymphocyte Ratio (PLR) as the Prognostic Factor for Recurrence/Residual Disease in HSIL Patients After LEEP.J Inflamm Res. 2023 May 1;16:1923-1936. doi: 10.2147/JIR.S406082. eCollection 2023. J Inflamm Res. 2023. PMID: 37152868 Free PMC article.
-
Prevalence and genotype distribution of human papillomavirus infection among women aged 30-65 years in Xi'an, China: a population-based study of 14,655 women.Hum Vaccin Immunother. 2021 Dec 2;17(12):5439-5446. doi: 10.1080/21645515.2021.2007709. Epub 2021 Dec 10. Hum Vaccin Immunother. 2021. PMID: 34893010 Free PMC article.
-
Use of extended HR-HPV Genotyping in improving the Triage Strategy of 2019 ASCCP recommendations in Women with positive HR-HPV diagnosis and Simultaneous LSIL Cytology Results.J Cancer. 2021 May 19;12(14):4332-4340. doi: 10.7150/jca.55826. eCollection 2021. J Cancer. 2021. PMID: 34093833 Free PMC article.
-
Classification and diagnosis of cervical lesions based on colposcopy images using deep fully convolutional networks: A man-machine comparison cohort study.Fundam Res. 2022 Nov 9;5(1):419-428. doi: 10.1016/j.fmre.2022.09.032. eCollection 2025 Jan. Fundam Res. 2022. PMID: 40166111 Free PMC article.
References
-
- International Agency for Research on Cancer. GLOBOCAN 2012: cancer fact sheet. Cervical cancer estimated incidence, mortality and prevalence worldwide in 2012 [Internet] Lyon: International Agency for Research on Cancer; 2013. [cited 2013 Dec 12]. Available from: http://globocan.iarc.fr/old/FactSheets/cancers/cervix-new.asp.
-
- Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65:87–108. - PubMed
-
- Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66:115–132. - PubMed
-
- Crosbie EJ, Einstein MH, Franceschi S, Kitchener HC. Human papillomavirus and cervical cancer. Lancet. 2013;382:889–899. - PubMed
