

Clinical diagnosis of TIA or minor stroke and prognosis in patients with neurological symptoms: A rapid access clinic cohort
- PMID: 30889185
- PMCID: PMC6424476
- DOI: 10.1371/journal.pone.0210452
Clinical diagnosis of TIA or minor stroke and prognosis in patients with neurological symptoms: A rapid access clinic cohort
Abstract
Background: The long-term risk of stroke or myocardial infarction (MI) in patients with minor neurological symptoms who are not clinically diagnosed with transient ischaemic attack (TIA) or minor stroke is uncertain.
Methods: We used data from a rapid access clinic for patients with suspected TIA or minor stroke and follow-up from four overlapping data sources for a diagnosis of ischaemic or haemorrhagic stroke, MI, major haemorrhage and death. We identified patients with and without a clinical diagnosis of TIA or minor stroke. We estimated hazard ratios of stroke, MI, major haemorrhage and death in early and late time periods.
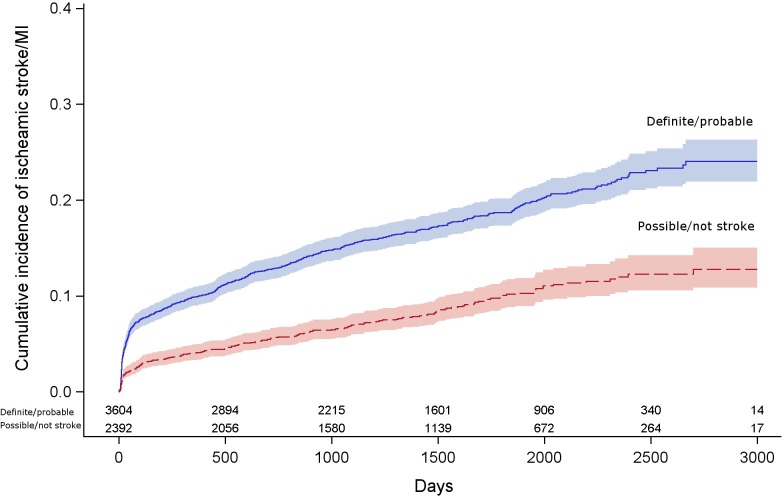
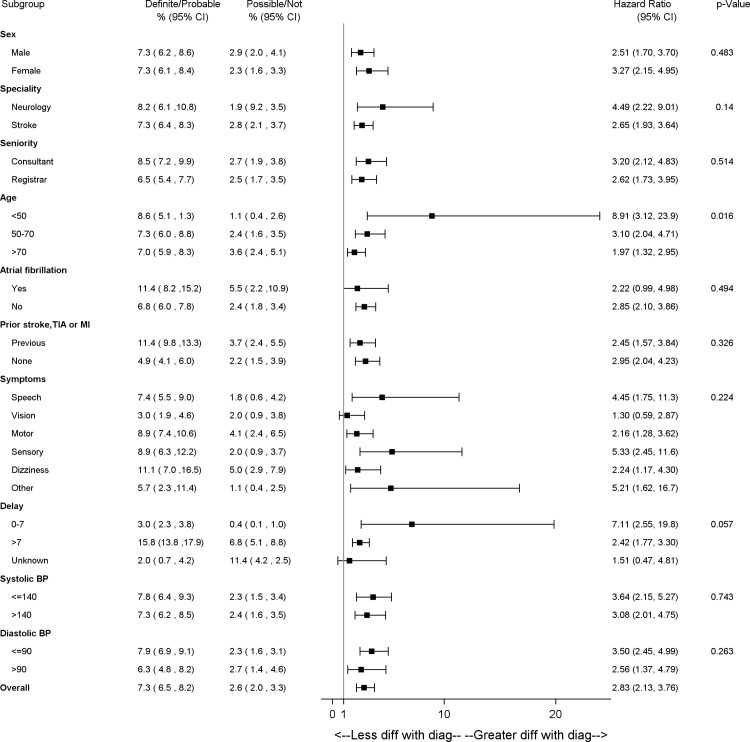
Results: 5,997 patients were seen from 2005-2013, who were diagnosed with TIA or minor stroke (n = 3604, 60%) or with other diagnoses (n = 2392, 40%). By 5 years the proportion of patients who had a subsequent ischaemic stroke or MI, in patients with a clinical diagnosis of minor stroke or TIA was 19% [95% confidence interval (CI): 17-20%], and in patients with other diagnoses was 10% (95%CI: 8-15%). Patients with clinical diagnosis of TIA or minor stroke had three times the hazard of stroke or MI compared to patients with other diagnoses [hazard ratio (HR)2.83 95%CI:2.13-3.76, adjusted age and sex] by 90 days post-event; however from 90 days to end of follow up, this difference was attenuated (HR 1.52, 95%CI:1.25-1.86). Older patients and those who had a history of vascular disease had a high risk of stroke or MI, whether or not they were diagnosed with minor stroke or TIA.
Conclusions: Careful attention to vascular risk factors in patients presenting with transient or minor neurological symptoms not thought to be due to stroke or TIA is justified, particularly those who are older or have a history of vascular disease.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Brazzelli M, Sandercock PAG, Chappell FM, Celani MG, Righetti E, Arestis N, et al. Magnetic resonance imaging versus computed tomography for detection of acute vascular lesions in patients presenting with stroke symptoms. CochraneDatabaseSystRev. 2008;CD007424 10.1002/14651858.CD007424 - DOI - PubMed
-
- Ferro JM, Falcao I, Rodrigues G, Canhao P, Melo TP, Oliveira V, et al. Diagnosis of transient ischemic attack by the nonneurologist. A validation study. Stroke. 1996;27: 2225–2229. - PubMed
-
- Kraaijeveld CL, van Gijn J, Schouten HJ, Staal A. Interobserver agreement for the diagnosis of transient ischemic attacks. Stroke. 1984;15: 723–725. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
