

Neuroimaging and connectomics of drug-resistant epilepsy at multiple scales: From focal lesions to macroscale networks
- PMID: 30889276
- PMCID: PMC6447443
- DOI: 10.1111/epi.14688
Neuroimaging and connectomics of drug-resistant epilepsy at multiple scales: From focal lesions to macroscale networks
Abstract
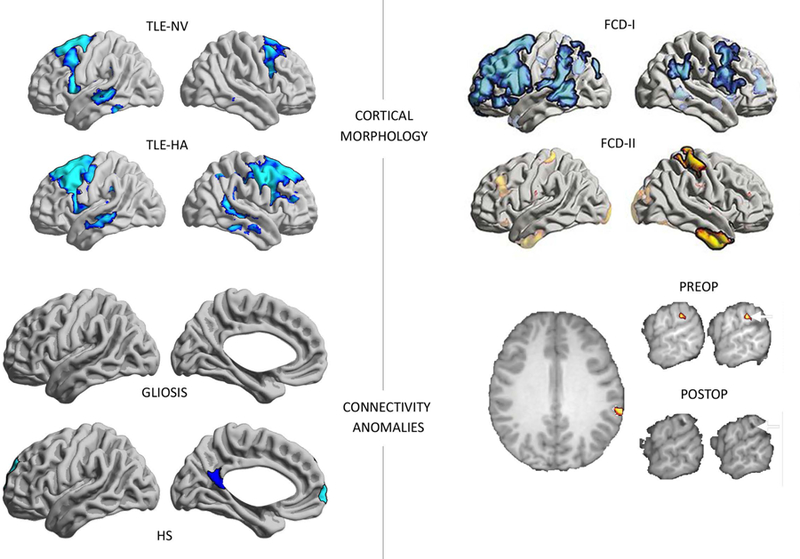
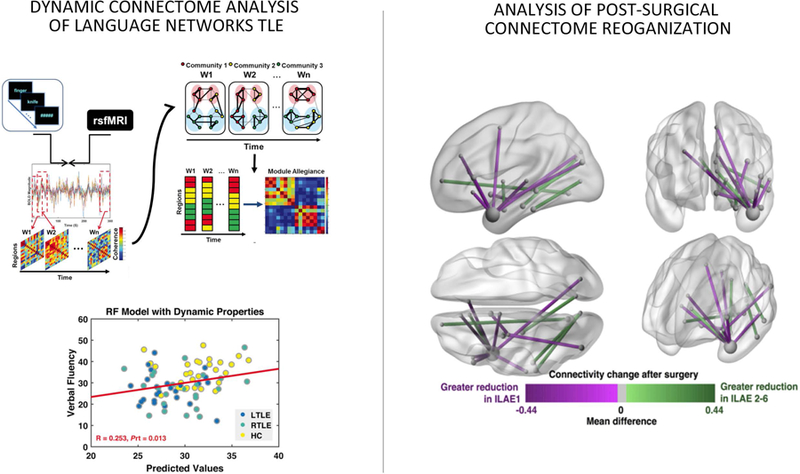
Epilepsy is among the most common chronic neurologic disorders, with 30%-40% of patients having seizures despite antiepileptic drug treatment. The advent of brain imaging and network analyses has greatly improved the understanding of this condition. In particular, developments in magnetic resonance imaging (MRI) have provided measures for the noninvasive characterization and detection of lesions causing epilepsy. MRI techniques can probe structural and functional connectivity, and network analyses have shaped our understanding of whole-brain anomalies associated with focal epilepsies. This review considers the progress made by neuroimaging and connectomics in the study of drug-resistant epilepsies due to focal substrates, particularly temporal lobe epilepsy related to mesiotemporal sclerosis and extratemporal lobe epilepsies associated with malformations of cortical development. In these disorders, there is evidence of widespread disturbances of structural and functional connectivity that may contribute to the clinical and cognitive prognosis of individual patients. It is hoped that studying the interplay between macroscale network anomalies and lesional profiles will improve our understanding of focal epilepsies and assist treatment choices.
Keywords: MRI; biomarker; connectivity; connectome; epilepsy.
Wiley Periodicals, Inc. © 2019 International League Against Epilepsy.
Conflict of interest statement
D
None of the authors has any conflict of interest to disclose.
Figures



References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
