

Neurocognitive SuperAging in Older Adults Living With HIV: Demographic, Neuromedical and Everyday Functioning Correlates
- PMID: 30890191
- PMCID: PMC6705613
- DOI: 10.1017/S1355617719000018
Neurocognitive SuperAging in Older Adults Living With HIV: Demographic, Neuromedical and Everyday Functioning Correlates
Abstract
Objectives: Studies of neurocognitively elite older adults, termed SuperAgers, have identified clinical predictors and neurobiological indicators of resilience against age-related neurocognitive decline. Despite rising rates of older persons living with HIV (PLWH), SuperAging (SA) in PLWH remains undefined. We aimed to establish neuropsychological criteria for SA in PLWH and examined clinically relevant correlates of SA.
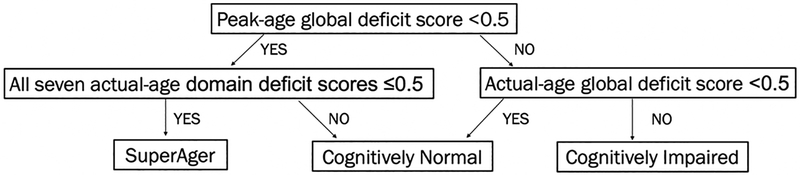
Methods: 734 PLWH and 123 HIV-uninfected participants between 50 and 64 years of age underwent neuropsychological and neuromedical evaluations. SA was defined as demographically corrected (i.e., sex, race/ethnicity, education) global neurocognitive performance within normal range for 25-year-olds. Remaining participants were labeled cognitively normal (CN) or impaired (CI) based on actual age. Chi-square and analysis of variance tests examined HIV group differences on neurocognitive status and demographics. Within PLWH, neurocognitive status differences were tested on HIV disease characteristics, medical comorbidities, and everyday functioning. Multinomial logistic regression explored independent predictors of neurocognitive status.
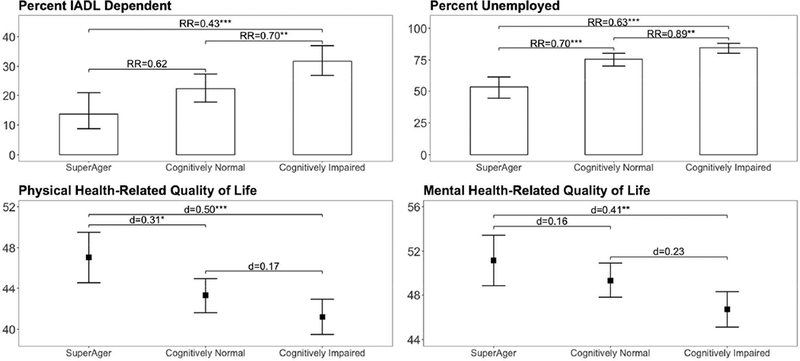
Results: Neurocognitive status rates and demographic characteristics differed between PLWH (SA=17%; CN=38%; CI=45%) and HIV-uninfected participants (SA=35%; CN=55%; CI=11%). In PLWH, neurocognitive groups were comparable on demographic and HIV disease characteristics. Younger age, higher verbal IQ, absence of diabetes, fewer depressive symptoms, and lifetime cannabis use disorder increased likelihood of SA. SA reported increased independence in everyday functioning, employment, and health-related quality of life than non-SA.
Conclusions: Despite combined neurological risk of aging and HIV, youthful neurocognitive performance is possible for older PLWH. SA relates to improved real-world functioning and may be better explained by cognitive reserve and maintenance of cardiometabolic and mental health than HIV disease severity. Future research investigating biomarker and lifestyle (e.g., physical activity) correlates of SA may help identify modifiable neuroprotective factors against HIV-related neurobiological aging. (JINS, 2019, 25, 507-519).
Keywords: Acquired Immunodeficiency Syndrome; Cannabis; Cognitive decline; Cognitive reserve; Diabetes; Neuropsychology.
Figures
References
-
- Beck A, Steer R, & Brown G (1996). Manual for Beck Depression Inventory II (BDI-II). San Antonio, TX, Psychology Corporation.
Publication types
MeSH terms
Grants and funding
- HHSN271201000030C/MH/NIMH NIH HHS/United States
- U24 MH100928/MH/NIMH NIH HHS/United States
- HHSN271201000036C/MH/NIMH NIH HHS/United States
- R24 MH059745/MH/NIMH NIH HHS/United States
- T32 DA031098/DA/NIDA NIH HHS/United States
- T32 AA013525/AA/NIAAA NIH HHS/United States
- P30 MH062512/MH/NIMH NIH HHS/United States
- U01 MH083506/MH/NIMH NIH HHS/United States
- F31 AA027198/AA/NIAAA NIH HHS/United States
- K24 MH097673/MH/NIMH NIH HHS/United States
- N01 MH022005/MH/NIMH NIH HHS/United States
- R01 MH099987/MH/NIMH NIH HHS/United States
- R01 MH107345/MH/NIMH NIH HHS/United States
- U24 MH100930/MH/NIMH NIH HHS/United States
