

A systematic literature review and meta-analysis of minimal residual disease as a prognostic indicator in adult B-cell acute lymphoblastic leukemia
- PMID: 30890593
- PMCID: PMC6886415
- DOI: 10.3324/haematol.2018.201053
A systematic literature review and meta-analysis of minimal residual disease as a prognostic indicator in adult B-cell acute lymphoblastic leukemia
Abstract
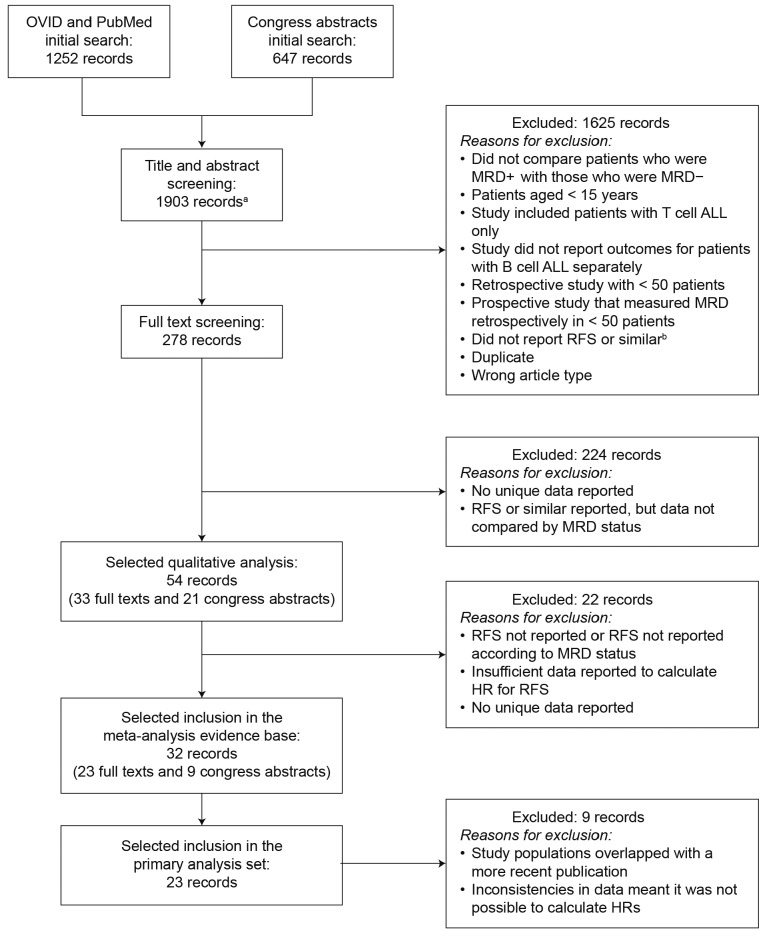
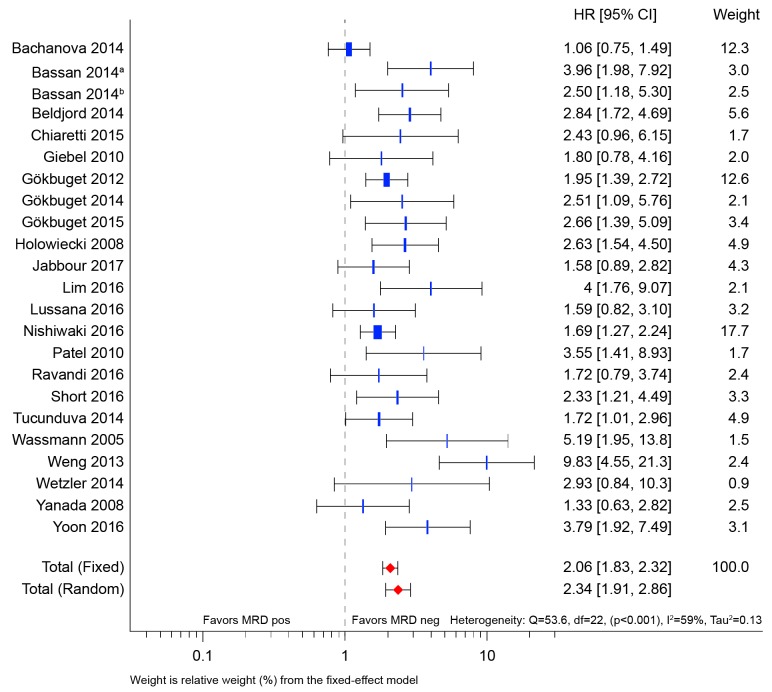
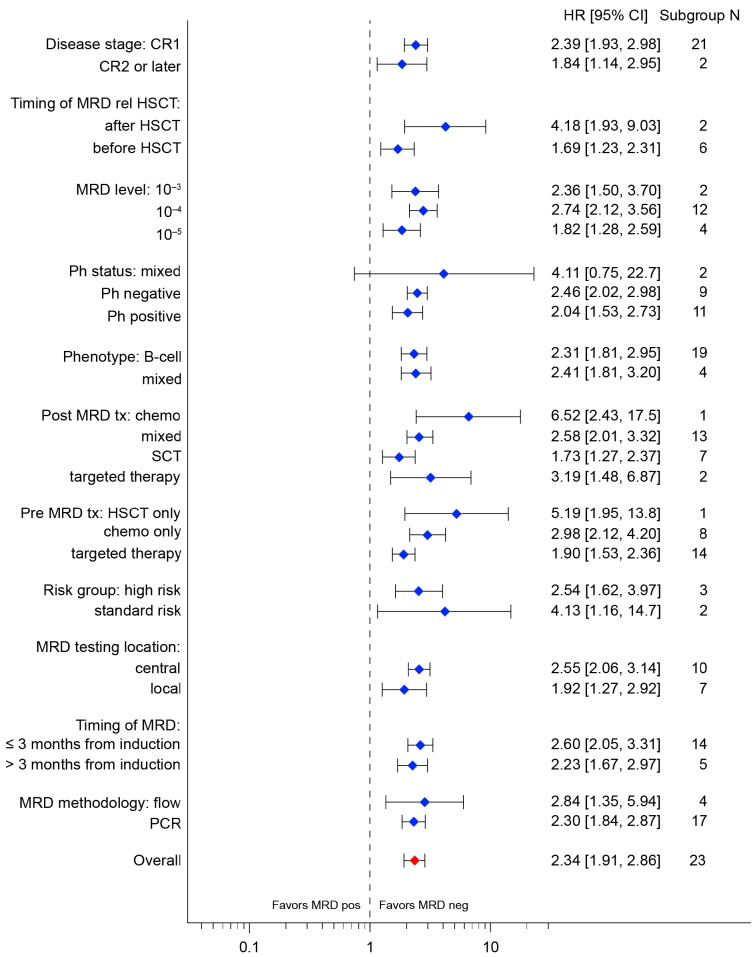
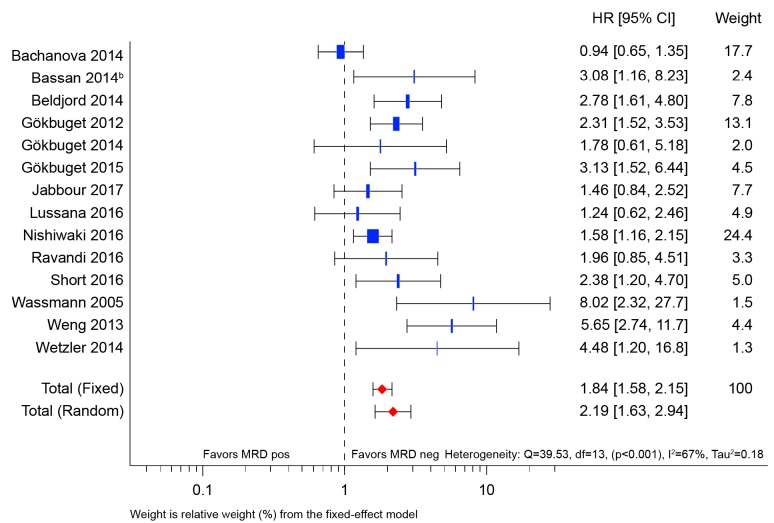
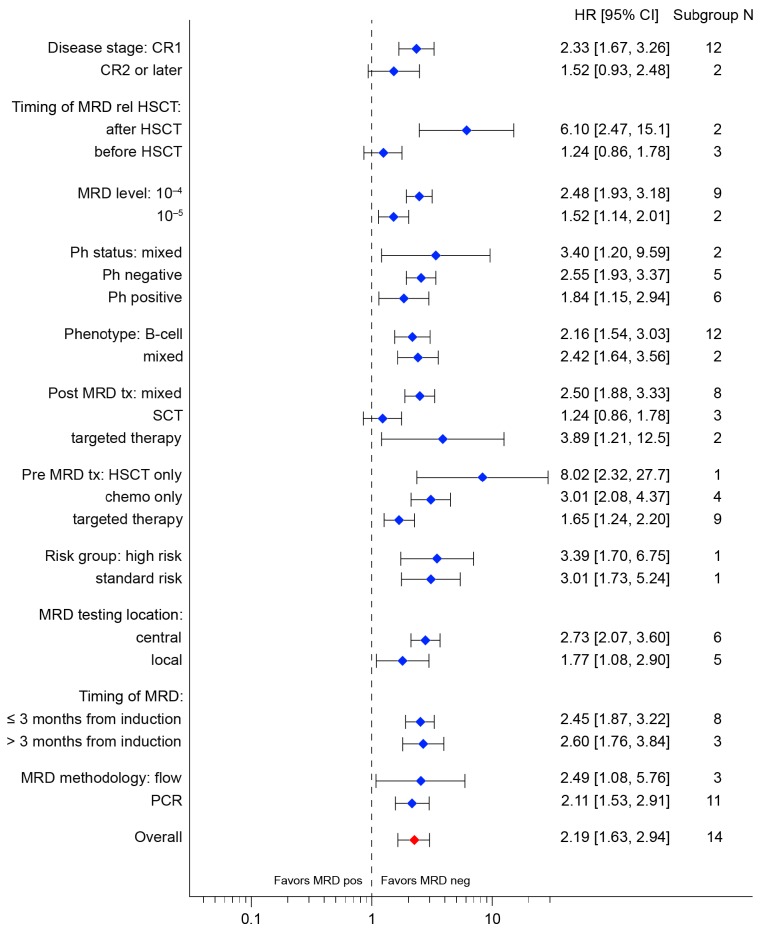
Minimal (or 'measurable') residual disease in acute lymphoblastic leukemia appears to be a prognostic indicator, with potential value in informing individualized treatment decisions. Complete understanding of the strength of the association between minimal residual disease and long-term outcomes is, however, lacking. A systematic literature review and meta-analysis were performed to elucidate the clinical significance of minimal residual disease with respect to relapse-free survival and overall survival in precursor B-cell acute lymphoblastic leukemia. A total of 23 articles and abstracts, most published between 2012 and 2016, were identified for inclusion in the primary meta-analysis. Typically, patients were in their first complete remission at the time of minimal residual disease assessment; in two studies, all patients were in their second, or later, complete remission. The primary analysis revealed improved relapse-free survival across all studies for patients who achieved minimal residual disease negativity (random effects hazard ratio, 2.34; 95% confidence interval, 1.91-2.86). Improved overall survival for patients who achieved minimal residual disease negativity was also observed (hazard ratio, 2.19; 95% confidence interval, 1.63-2.94). There was no observed difference in the impact of minimal residual disease status in subgroups based on disease stage, minimal residual disease sensitivity threshold level, Philadelphia chromosome status, histological phenotype, risk group, minimal residual disease testing location, minimal residual disease timing after induction, or minimal residual disease detection method. Despite heterogeneity in study design and patient populations between the contributing studies, these data provide a compelling argument for minimal residual disease as a clinical tool for assessing prognosis and guiding treatment decisions in precursor B-cell acute lymphoblastic leukemia.
Copyright© 2019 Ferrata Storti Foundation.
Figures
References
-
- Carroll W, Loh M, Biondi A, Willman C. The biology of acute lymphoblastic leukemia In: Reaman G, Smith F, eds. Childhood Leukemia: a Practical Handbook. Berlin and Heidelberg: Springer-Verlag; 2011:29–61.
-
- Cancer Research UK. Types of acute lymphoblastic leukaemia. 2015. Available from: http://www.cancerresearchuk.org/about-cancer/acute-lymphoblastic-leukaem... (Accessed 24 May 2016).
-
- Fielding AK. Current treatment of Philadelphia chromosome-positive acute lymphoblastic leukemia. Hematology Am Soc Hematol Educ Program. 2011;2011(1): 231–237. - PubMed
-
- Faderl S, Kantarjian HM, Talpaz M, Estrov Z. Clinical significance of cytogenetic abnormalities in adult acute lymphoblastic leukemia. Blood. 1998;91(11):3995–4019. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
