

Transsphenoidal versus Transcranial Approach for Treatment of Tuberculum Sellae Meningiomas: A Systematic Review and Meta-analysis of Comparative Studies
- PMID: 30890739
- PMCID: PMC6424979
- DOI: 10.1038/s41598-019-41292-0
Transsphenoidal versus Transcranial Approach for Treatment of Tuberculum Sellae Meningiomas: A Systematic Review and Meta-analysis of Comparative Studies
Abstract
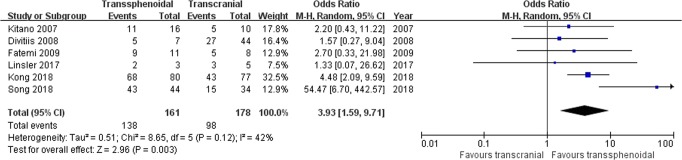
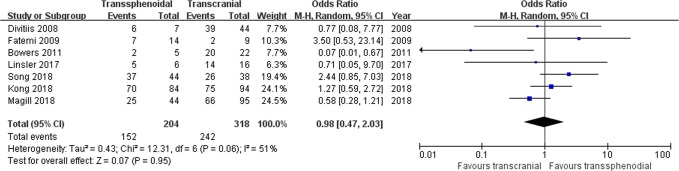
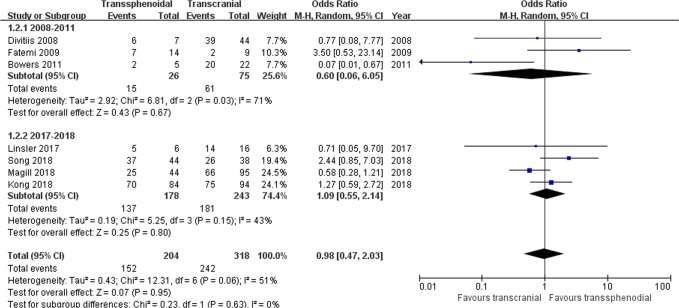
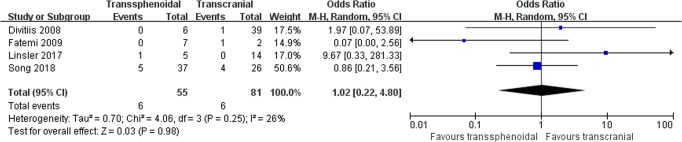
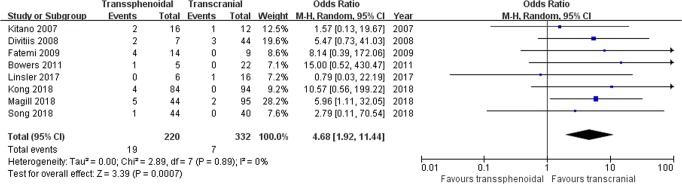
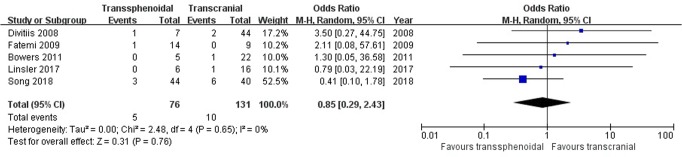
There is controversy regarding the surgical route selection for tuberculum sellae meningiomas (TSMs): the transsphenoidal (TS) or transcranial (TC) approach? We conducted a systematic review and meta-analysis to compare clinical outcomes and postoperative complications between two surgical approaches. Literature search was performed. Relevant articles were selected and evaluated. Data were extracted and analyzed. Eight articles comprising 550 patients met the inclusion criteria. Traditionally, the rates of gross total resection, tumor recurrence, visual improvement, and cerebrospinal fluid leakage were the most common outcomes of interest. We demonstrated that the TS approach was significantly associated with better visual outcomes but more frequent cerebrospinal fluid leakage, while the rates of tumor resection and recurrence showed no significant difference between groups. In addition to surgical results that were consistent with previous studies, we further evaluated the impact of approach selection on common postoperative complications, which were closely related to the recovery course and quality of life. We revealed that the risk of dysosmia was significantly higher in the TS group. There was no significant difference between groups regarding infection, intracranial hemorrhage, and endocrine disorders. Because of the relatively low evidence levels of included retrospective studies, it was difficult to reach a categorical conclusion about the optimal surgical approach for TSMs. Finally, we recommended that the TS approach was an alternative option in patients with smaller TSMs (<30 mm) and limited invasion of optic canals in experienced neurosurgical centers.
Conflict of interest statement
The authors declare no competing interests.
Figures




References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
