

A case of pseudocystic liver metastases from an atypical lung carcinoid tumor
- PMID: 30891110
- PMCID: PMC6406078
- DOI: 10.1016/j.radcr.2019.02.022
A case of pseudocystic liver metastases from an atypical lung carcinoid tumor
Abstract
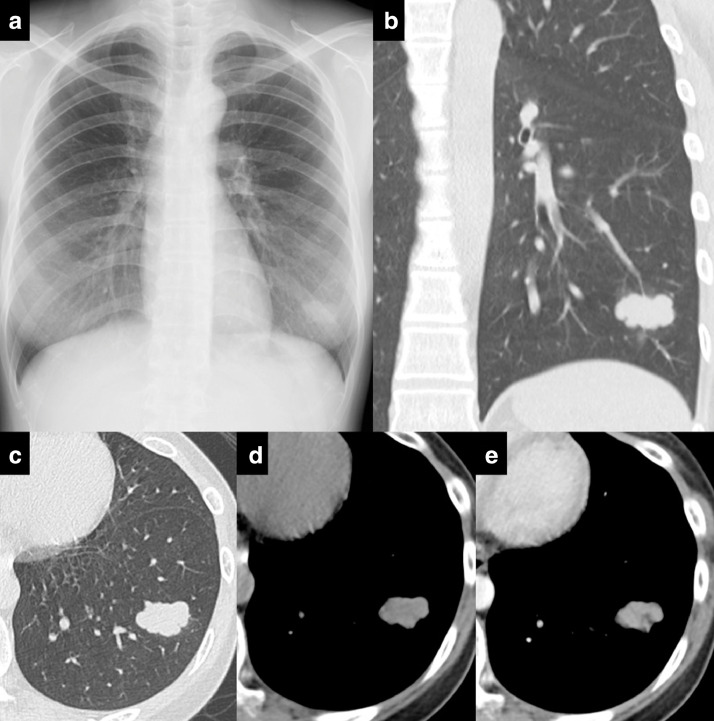
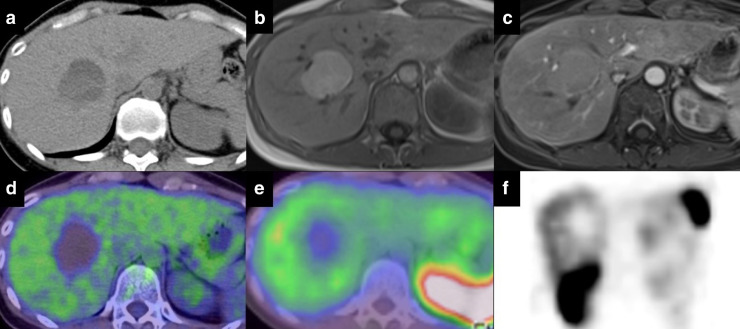
Metastatic neuroendocrine tumors of the liver typically appear as solid, hypervascular masses on imaging. Pseudocysts mimicking simple cysts are extremely rare. A 42-year-old Japanese woman was referred with a single pulmonary mass in the left lower lobe. No metastatic lesion was detected and no occupying lesion in the liver was observed. The lung tumor was diagnosed as an atypical carcinoid. Postoperative investigation revealed new hepatic simple cysts in the liver, which increased in size over time and changed into hemorrhagic cysts. Fluorodeoxyglucose positron emission tomography and somatostatin receptor scintigraphy using 111In-octreotide demonstrated no accumulation in the liver. Our patient did not have symptoms consistent with carcinoid syndrome. The patient underwent partial resection of the cystic lesions of the liver. Gross examination of the tumors demonstrated thin-wall cavitated lesions with hemorrhage which were metastases from the atypical carcinoid of the lung. When a growing cystic lesion with intracystic hemorrhage is found in the liver of a patient with a history of carcinoid tumors, pseudocysts caused by degeneration of a carcinoid metastasis should be considered as a differential diagnosis.
Keywords: Carcinoid metastasis; Liver metastasis; Lung carcinoid tumor; Neuroendocrine tumor; Pseudocyst.
Figures





Similar articles
-
Hepatic surgery for metastases from neuroendocrine tumors.Surg Oncol Clin N Am. 2003 Jan;12(1):231-42. doi: 10.1016/s1055-3207(02)00076-5. Surg Oncol Clin N Am. 2003. PMID: 12735141 Review.
-
Rare case of rectal carcinoid with synchronous primary carcinoid tumors of the lung misdiagnosed as lung metastases.JGH Open. 2024 Jul 19;8(7):e70003. doi: 10.1002/jgh3.70003. eCollection 2024 Jul. JGH Open. 2024. PMID: 39036414 Free PMC article.
-
[Multimodal therapy improved carcinoid syndrome secondary to liver metastases of an atypical lung carcinoid tumor:a case report].Nihon Shokakibyo Gakkai Zasshi. 2020;117(7):635-645. doi: 10.11405/nisshoshi.117.635. Nihon Shokakibyo Gakkai Zasshi. 2020. PMID: 32655123 Japanese.
-
Multiple liver metastases of pulmonary carcinoid successfully treated by two-stage hepatectomy combined with embolization of portal vein branches: Report of a case.Int J Surg Case Rep. 2020;71:319-322. doi: 10.1016/j.ijscr.2020.05.043. Epub 2020 May 29. Int J Surg Case Rep. 2020. PMID: 32492643 Free PMC article.
-
Hepatic pseudocystic metastasis of well-differentiated ileal neuroendocrine tumor: a case report with review of the literature.Diagn Pathol. 2013 Sep 13;8:148. doi: 10.1186/1746-1596-8-148. Diagn Pathol. 2013. PMID: 24034980 Free PMC article. Review.
Cited by
-
Liver metastasis mimicking an abscess.BJR Case Rep. 2021 Apr 12;7(4):20200201. doi: 10.1259/bjrcr.20200201. eCollection 2021 Jul 16. BJR Case Rep. 2021. PMID: 35047196 Free PMC article.
-
Liver metastasis or a pseudocyst? A rare presentation of leiomyosarcoma's metastasis in the liver.Contemp Oncol (Pozn). 2022;26(4):306-309. doi: 10.5114/wo.2022.124595. Epub 2022 Dec 30. Contemp Oncol (Pozn). 2022. PMID: 36816396 Free PMC article.
-
Hyperechogenicity and histopathological features of focal liver lesions.J Med Ultrason (2001). 2025 Jan;52(1):55-67. doi: 10.1007/s10396-024-01475-3. Epub 2024 Jul 3. J Med Ultrason (2001). 2025. PMID: 38958787 Review.
References
-
- Hendifar A.E., Marchevsky A.M., Tuli R. Neuroendocrine tumors of the lung: current challenges and advances in the diagnosis and management of well-differentiated disease. J Thorac Oncol. 2016;12(3):425–436. - PubMed
-
- Travis W.D., Brambilla E., Burke A.P., Marx A., Nicolson A.G. 4th ed. International Agency for Research on Cancer; Lyon, France: 2015. WHO classification of tumours of the lung, pleura, thymus and heart. - PubMed
-
- Chong S., Lee K.S., Chung M.J., Han J., Kwon O.J., Kim T.S. Neuroendocrine tumors of the lung: clinical, pathologic, and imaging findings. Radiographics. 2006;26(1):41–58. - PubMed
-
- Baxi A.J., Chintapalli K., Katkar A., Restrepo C.S., Betancourt S.L., Sunnapwar A. Multimodality imaging findings in carcinoid tumors: a head-to-toe spectrum. Radiographics. 2017;37(2):516–536. - PubMed
-
- Scarsbrook A.F., Ganeshan A., Statham J., Thakker R.V., Weaver A., Talbot D. Anatomic and functional imaging of metastatic carcinoid tumors. Radiographics. 2007;27(2):455–477. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
