

Surgery for scar revision and reduction: from primary closure to flap surgery
- PMID: 30891462
- PMCID: PMC6404336
- DOI: 10.1186/s41038-019-0144-5
Surgery for scar revision and reduction: from primary closure to flap surgery
Abstract
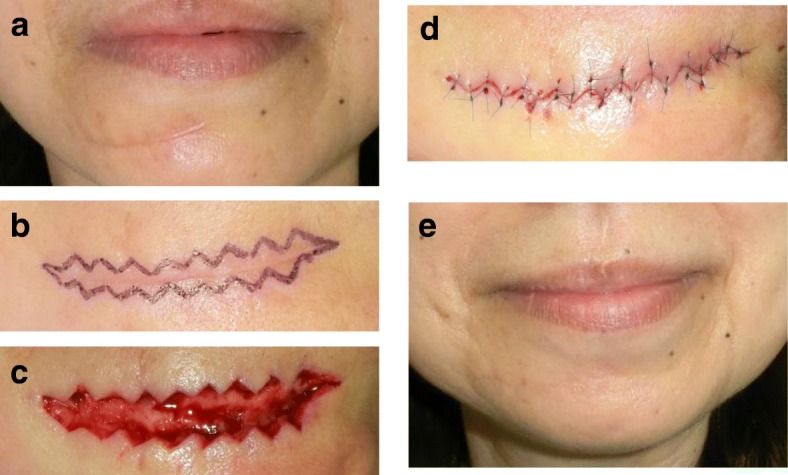
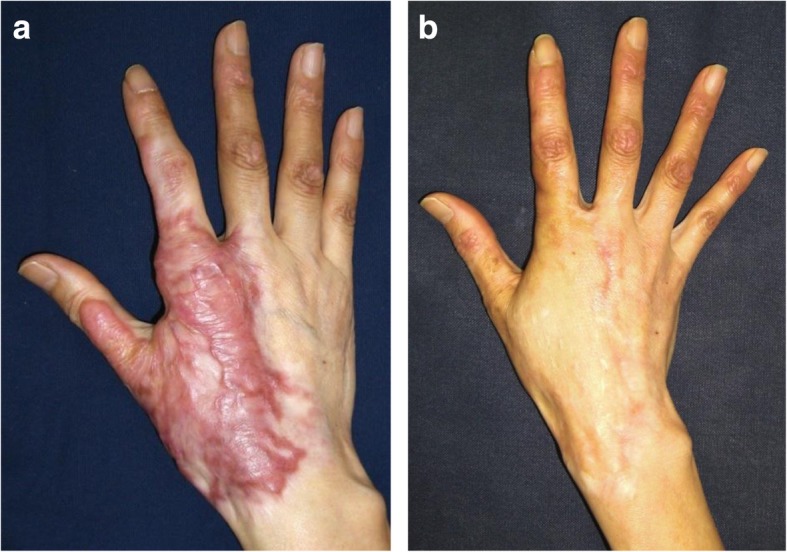
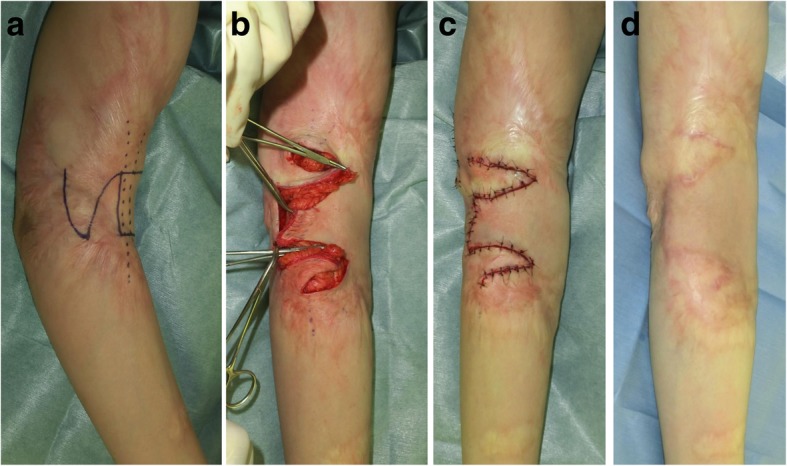
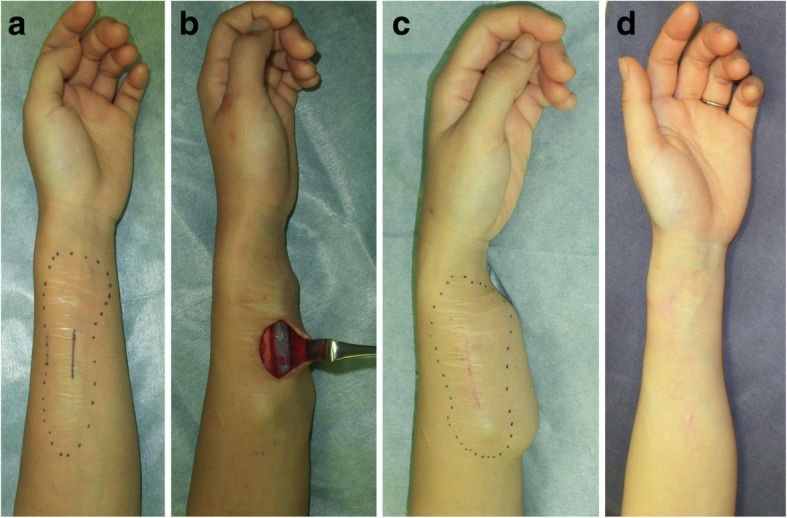
Scars are the final result of the four processes that constitute cutaneous wound healing, namely, coagulation, inflammation, proliferation, and remodeling. Permanent scars are produced if the wounds reach the reticular dermis. The nature of these scars depends on the four wound healing processes. If the remodeling process is excessive, collagen degradation exceeds collagen synthesis and atrophic scars are produced. If the inflammation phase is prolonged and/or more potent for some reason, inflammatory/pathological scars such as keloids or hypertrophic scars can arise. If these pathological scars are located on joints or mobile regions, scar contractures can develop. When used with the appropriate timing and when selected on the basis of individual factors, surgical techniques can improve mature scars. This review paper focuses on the surgical techniques that are used to improve mature scars, burn scars, and scar contractures. Those methods include z-plasties, w-plasties, split-thickness skin grafting, full-thickness skin grafting, local flaps (including the square flap method and the propeller flap), and expanded flaps, distant flaps, regional flaps, and free flaps.
Keywords: Expander; Hypertrophic scar; Keloid; Local flap; Perforator flap; Scar; Scar contracture; Surgery; W-plasty; Z-plasty.
Conflict of interest statement
Consent for inclusion in the Nippon Medical School Hospital Registry includes the possibility of publication of information for research purposes.The author declares that he has no competing interests.
Figures





References
-
- Dunkin CS, Pleat JM, Gillespie PH, Tyler MP, Roberts AH, McGrouther DA. Scarring occurs at a critical depth of skin injury: precise measurement in a graduated dermal scratch in human volunteers. Plast Reconstr Surg. 2007;119(6):1722–1732. - PubMed
-
- Orgill DP, Ogawa R. Current methods of burn reconstruction. Plast Reconstr Surg. 2013;131(5):827e–836e. - PubMed
-
- Ogawa R, Akaishi S, Kuribayashi S, Miyashita T. Keloids and hypertrophic scars can now be cured completely: recent progress in our understanding of the pathogenesis of keloids and hypertrophic scars and the most promising current therapeutic strategy. J Nippon Med Sch. 2016;83(2):46–53. - PubMed
-
- Longacre JJ, Berry HK, Basom CR, Townsend SF. The effects of Z plasty on hypertrophic scars. Scand J Plast Reconstr Surg. 1976;10(2):113–128. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
