

Impact of Microscopic and Submicroscopic Parasitemia During Pregnancy on Placental Malaria in a High-Transmission Setting in Uganda
- PMID: 30891605
- PMCID: PMC6941619
- DOI: 10.1093/infdis/jiz130
Impact of Microscopic and Submicroscopic Parasitemia During Pregnancy on Placental Malaria in a High-Transmission Setting in Uganda
Abstract
Background: Placental malaria is a major cause of adverse birth outcomes. However, data are limited on the relationships between longitudinal measures of parasitemia during pregnancy and placental malaria.
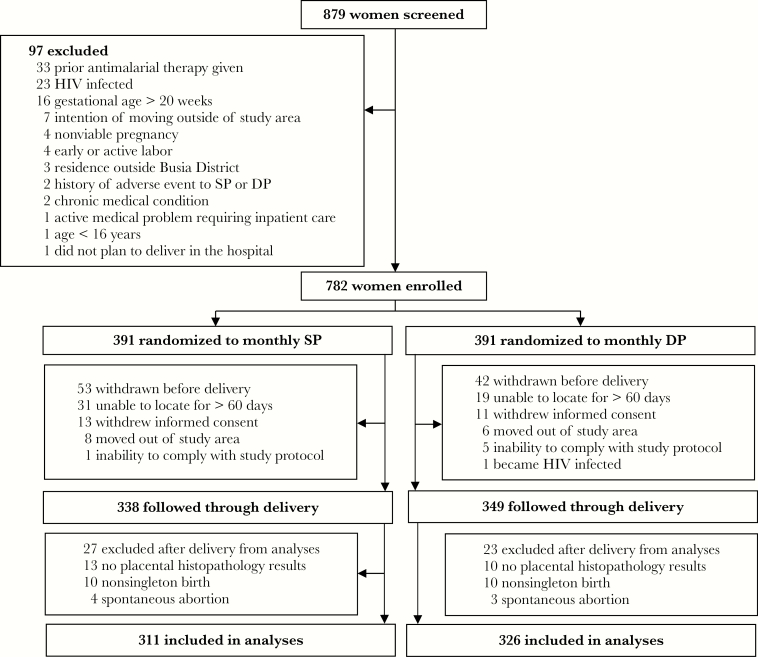
Methods: Data came from 637 women enrolled in a randomized controlled trial of intermittent preventive treatment of malaria in pregnancy (IPTp) from Uganda. Plasmodium falciparum parasitemia was assessed using microscopy and ultrasensitive quantitative PCR at intervals of 28 days from 12 to 20 weeks gestation through delivery. Multivariate analysis was used to measure associations between characteristics of parasitemia during pregnancy and the risk of placental malaria based on histopathology.
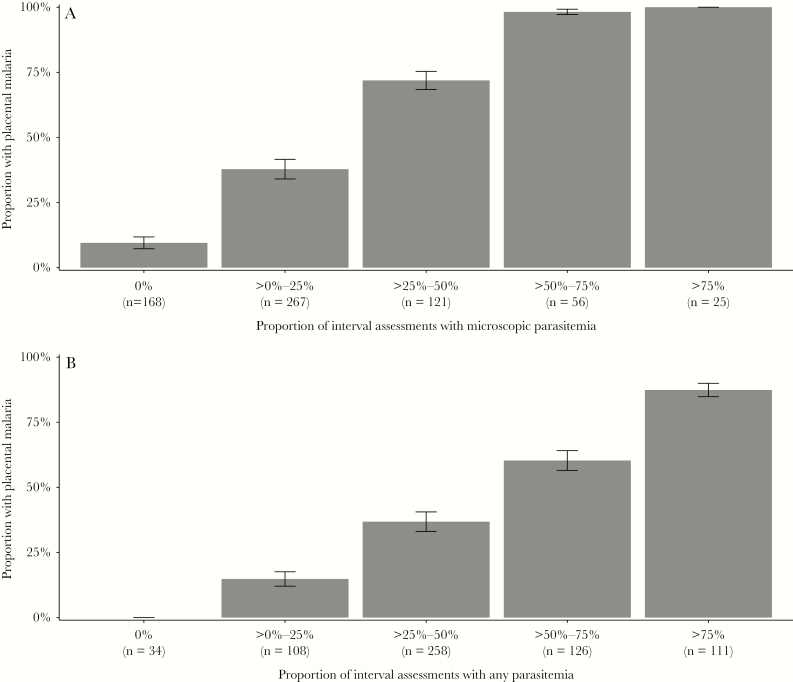
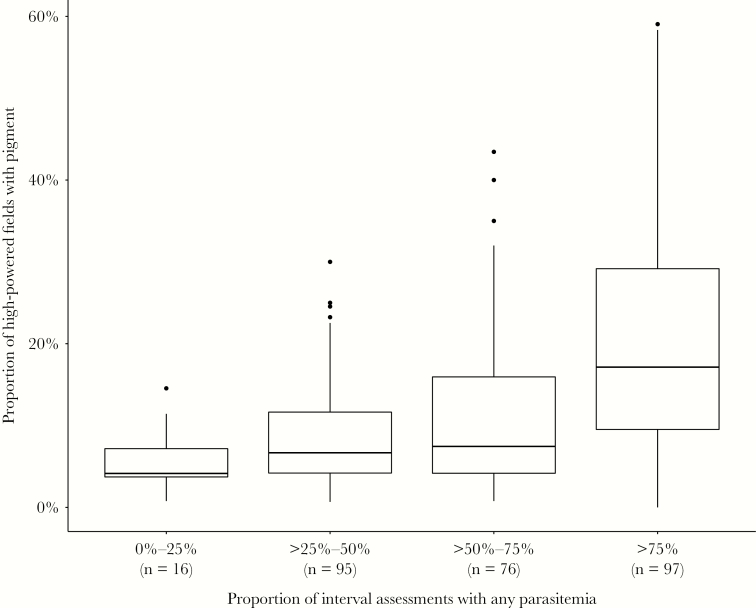
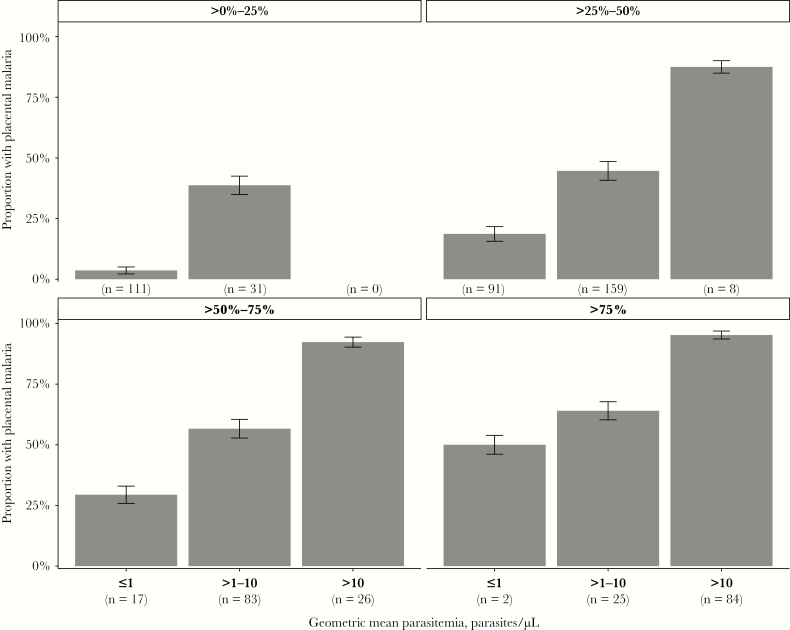
Results: Overall risk of placental malaria was 44.6%. None of the 34 women without parasitemia detected during pregnancy had evidence of placental malaria. Increasing proportion of interval assessments with parasitemia and higher parasite densities were independently associated with an increased risk of placental malaria. Higher gravidity and more effective IPTp were associated with a decreased risk of placental malaria. Women with parasitemia only detected before the third trimester still had an increased risk of placental malaria.
Conclusions: The frequency, density, and timing of parasitemia are all important risk factors for placental malaria. Interventions should target the prevention of all levels of parasitemia throughout pregnancy.
Keywords: asymptomatic malaria infection; dihydroartemisinin-piperaquine; intermittent preventive treatment during pregnancy; microscopic parasitemia; placental malaria; submicroscopic parasitemia.
© The Author(s) 2019. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
Similar articles
-
Relationships between infection with Plasmodium falciparum during pregnancy, measures of placental malaria, and adverse birth outcomes.Malar J. 2017 Oct 5;16(1):400. doi: 10.1186/s12936-017-2040-4. Malar J. 2017. PMID: 28982374 Free PMC article.
-
Decrease of microscopic Plasmodium falciparum infection prevalence during pregnancy following IPTp-SP implementation in urban cities of Gabon.Trans R Soc Trop Med Hyg. 2016 Jun;110(6):333-42. doi: 10.1093/trstmh/trw034. Epub 2016 Jun 6. Trans R Soc Trop Med Hyg. 2016. PMID: 27268713
-
The impact of gravidity, symptomatology and timing of infection on placental malaria.Malar J. 2020 Jun 24;19(1):227. doi: 10.1186/s12936-020-03297-3. Malar J. 2020. PMID: 32580739 Free PMC article. Clinical Trial.
-
Impact of Plasmodium falciparum malaria and intermittent preventive treatment of malaria in pregnancy on the risk of malaria in infants: a systematic review.Malar J. 2019 Sep 3;18(1):304. doi: 10.1186/s12936-019-2943-3. Malar J. 2019. PMID: 31481075 Free PMC article.
-
Malaria prevention in pregnancy, birthweight, and neonatal mortality: a meta-analysis of 32 national cross-sectional datasets in Africa.Lancet Infect Dis. 2012 Dec;12(12):942-9. doi: 10.1016/S1473-3099(12)70222-0. Epub 2012 Sep 18. Lancet Infect Dis. 2012. PMID: 22995852 Review.
Cited by
-
Age-modified factors associated with placental malaria in rural Burkina Faso.BMC Pregnancy Childbirth. 2022 Mar 24;22(1):248. doi: 10.1186/s12884-022-04568-4. BMC Pregnancy Childbirth. 2022. PMID: 35331181 Free PMC article. Clinical Trial.
-
The immune response to malaria in utero.Immunol Rev. 2020 Jan;293(1):216-229. doi: 10.1111/imr.12806. Epub 2019 Sep 25. Immunol Rev. 2020. PMID: 31553066 Free PMC article. Review.
-
Increased peripartum mortality associated with maternal subclinical malaria in Mozambique.Malar J. 2023 Jun 12;22(1):182. doi: 10.1186/s12936-023-04613-3. Malar J. 2023. PMID: 37309000 Free PMC article.
-
Piperaquine-Induced QTc Prolongation Decreases With Repeated Monthly Dihydroartemisinin-Piperaquine Dosing in Pregnant Ugandan Women.Clin Infect Dis. 2022 Aug 31;75(3):406-415. doi: 10.1093/cid/ciab965. Clin Infect Dis. 2022. PMID: 34864925 Free PMC article. Clinical Trial.
-
Association of malaria and curable sexually transmitted infections with pregnancy outcomes in rural Burkina Faso.BMC Pregnancy Childbirth. 2021 Oct 27;21(1):722. doi: 10.1186/s12884-021-04205-6. BMC Pregnancy Childbirth. 2021. PMID: 34706705 Free PMC article.
References
-
- Desai M, ter Kuile FO, Nosten F, et al. . Epidemiology and burden of malaria in pregnancy. Lancet Infect Dis 2007; 7:93–104. - PubMed
-
- Chico RM, Mayaud P, Ariti C, Mabey D, Ronsmans C, Chandramohan D. Prevalence of malaria and sexually transmitted and reproductive tract infections in pregnancy in sub-Saharan Africa: a systematic review. JAMA 2012; 307:2079–86. - PubMed
-
- van Geertruyden JP, Thomas F, Erhart A, D’Alessandro U. The contribution of malaria in pregnancy to perinatal mortality. Am J Trop Med Hyg 2004; 71:35–40. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
