

Biomarkers of Macrophage Activation and Immune Danger Signals Predict Clinical Outcomes in Alcoholic Hepatitis
- PMID: 30891779
- PMCID: PMC6752989
- DOI: 10.1002/hep.30617
Biomarkers of Macrophage Activation and Immune Danger Signals Predict Clinical Outcomes in Alcoholic Hepatitis
Abstract
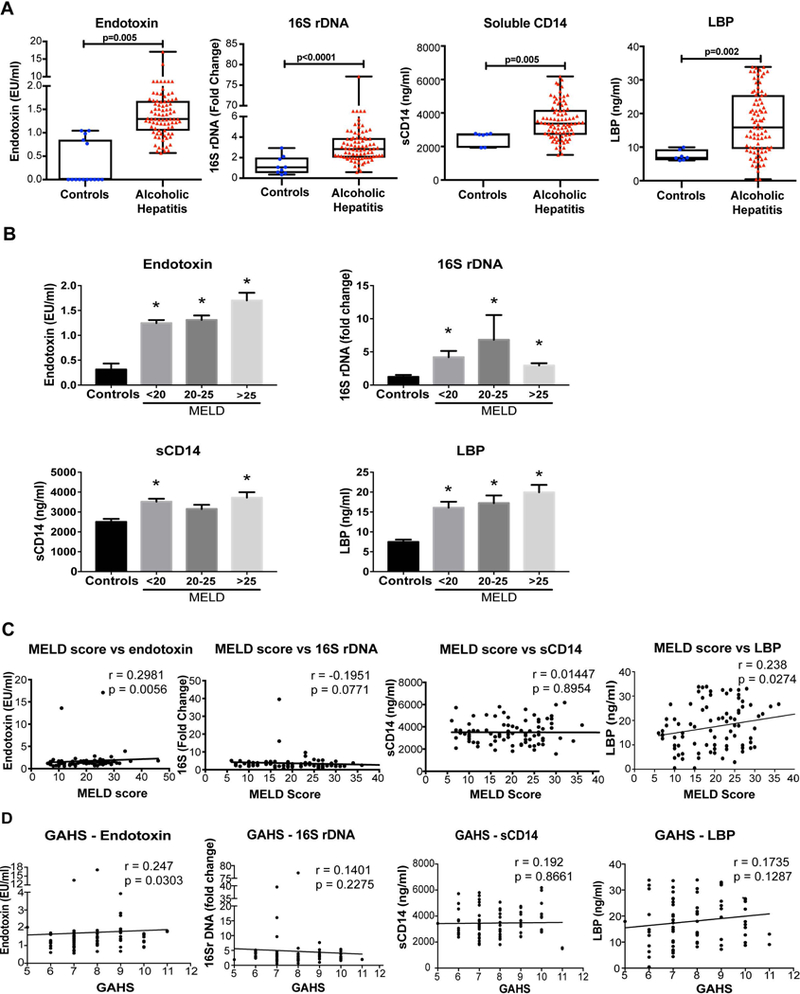
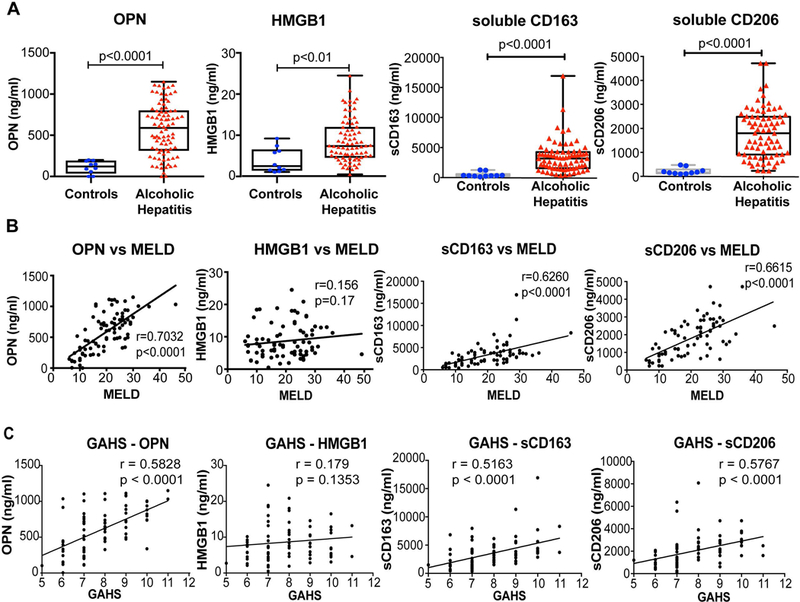
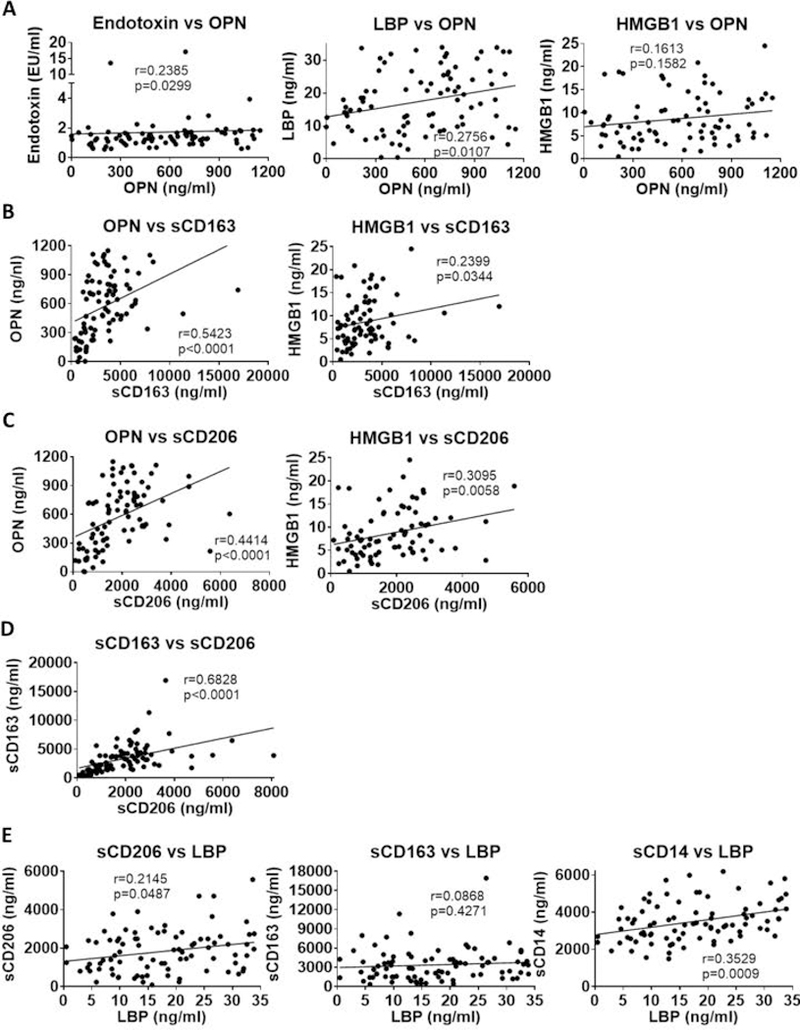
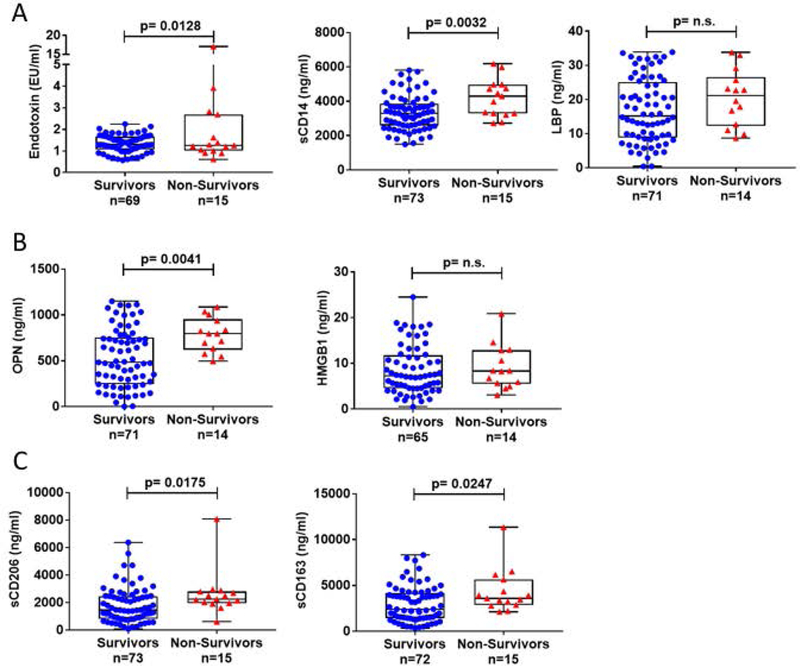
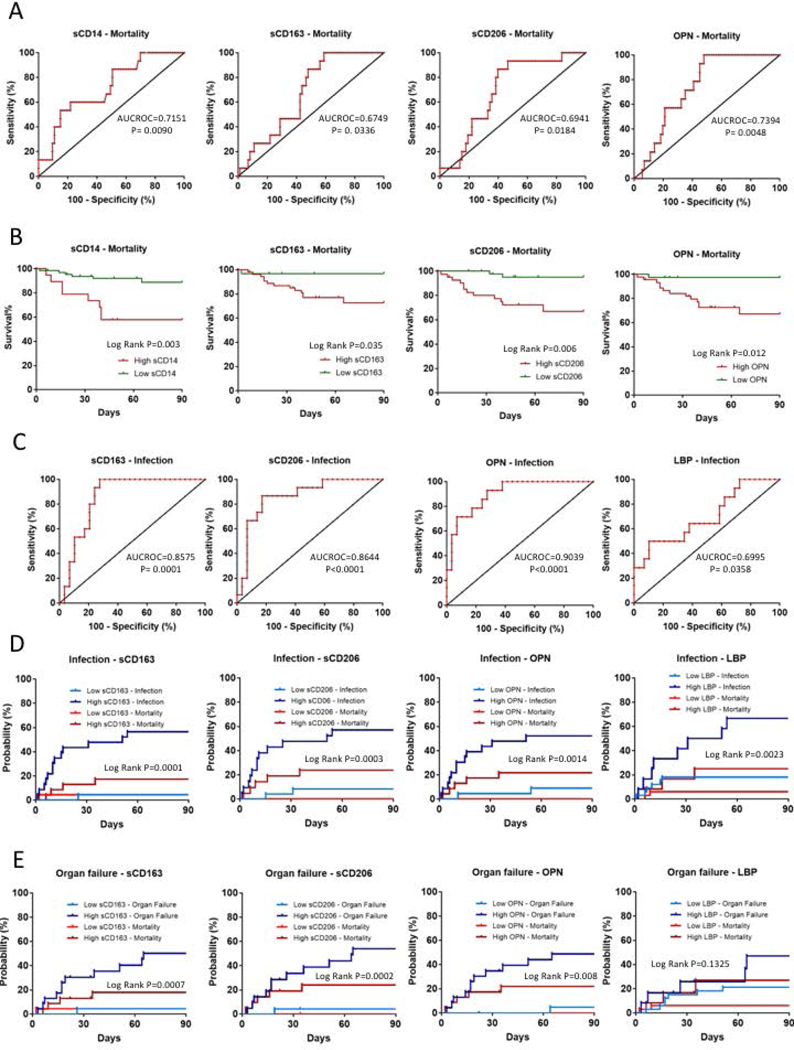
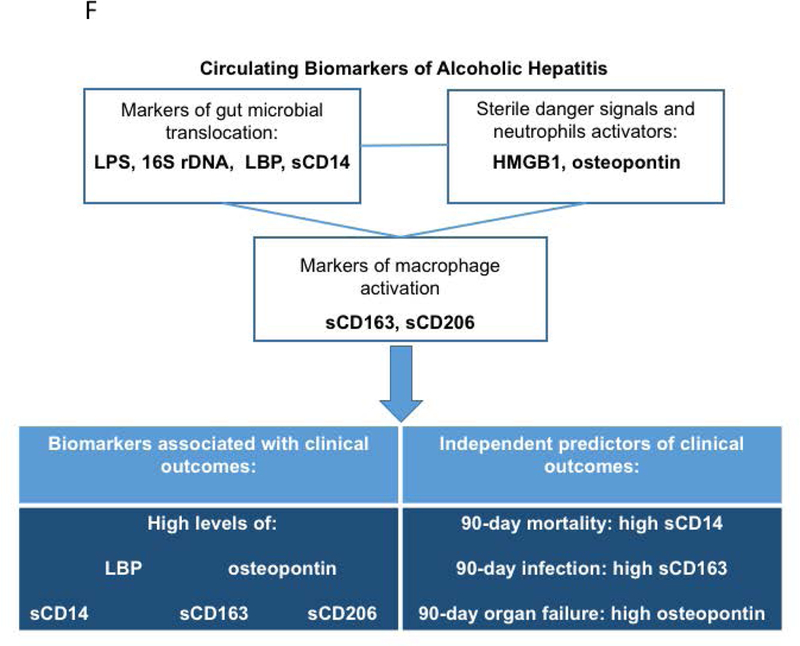
Although mortality due to acute alcoholic hepatitis (AH) correlates with Model for End-Stage Liver Disease (MELD) scores, biomarkers are critically needed to manage this disease. Increases in inflammatory markers and macrophage activation are associated with acute AH and could be potential biomarkers of clinical events and/or mortality. We enrolled 89 clinically diagnosed AH patients in four US academic medical centers. Plasma from AH patients had a significant increase in gut microbial translocation indicators (endotoxin, bacterial 16S ribosomal DNA) and host response indicators (soluble cluster of differentiation 14 [sCD14] and lipopolysaccharide binding protein [LBP]) compared to controls. Patient MELD score and Glasgow Alcoholic Hepatitis score (GAHS) correlated with endotoxin levels. AH patients also had a significant increase in high mobility group protein 1 (HMGB1), a sterile danger signal molecule, and osteopontin (OPN), a multifunctional phosphoprotein involved in neutrophil activation, compared to controls. Increased levels of OPN positively correlated with increasing MELD score, GAHS, and LBP levels. Consistent with these results, AH patients had significantly increased circulating levels of macrophage activation (sCD163 and sCD206) markers compared to healthy controls, and sCD163 and sCD206 significantly and positively correlated with OPN, HMGB1, and LBP levels as well as with MELD score and GAHS. These findings indicate a connection between microbial translocation, immune cell activation, and AH severity. Plasma sCD14, OPN, sCD163, and sCD206 levels were significantly higher in nonsurvivors than survivors. In multivariate regression models, we identified sCD14, sCD163, and OPN as independent predictors of 90-day mortality, infection, and organ failure development, respectively. Conclusion: Our study suggests that sCD14, LBP, OPN, sCD163, and sCD206 are biomarkers to indicate severity and predict clinical outcomes in AH.
© 2019 by the American Association for the Study of Liver Diseases.
Figures
References
-
- Rehm J, Samokhvalov AV, Shield KD. Global burden of alcoholic liver diseases. J Hepatol 2013;59:160–168. - PubMed
-
- EASL Clinical Practice Guidelines: Management of alcohol-related liver disease. J Hepatol 2018;69:154–181. - PubMed
-
- Lucey MR, Mathurin P, Morgan TR. Alcoholic hepatitis. N Engl J Med 2009;360:2758–2769. - PubMed
-
- Enomoto N, Ikejima K, Bradford BU, Rivera CA, Kono H, Goto M, Yamashina S, et al. Role of Kupffer cells and gut-derived endotoxins in alcoholic liver injury. J Gastroenterol Hepatol 2000;15 Suppl:D20–25. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 AA011576/AA/NIAAA NIH HHS/United States
- P20 GM113226/GM/NIGMS NIH HHS/United States
- UL1 TR002548/TR/NCATS NIH HHS/United States
- U01 AA026933/AA/NIAAA NIH HHS/United States
- U01 AA021902/AA/NIAAA NIH HHS/United States
- U01 AA026976/AA/NIAAA NIH HHS/United States
- R01 AA023681/AA/NIAAA NIH HHS/United States
- R01 DK113196/DK/NIDDK NIH HHS/United States
- U01 AA021907/AA/NIAAA NIH HHS/United States
- P50 AA024333/AA/NIAAA NIH HHS/United States
- U01 AA026975/AA/NIAAA NIH HHS/United States
- I01 BX002996/BX/BLRD VA/United States
- U01 AA021893/AA/NIAAA NIH HHS/United States
- U01 AA021901/AA/NIAAA NIH HHS/United States
- R01 GM119174/GM/NIGMS NIH HHS/United States
- P50 AA024337/AA/NIAAA NIH HHS/United States
- R21 AR071046/AR/NIAMS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
