

Early combined immunosuppression may be effective and safe in older patients with Crohn's disease: post hoc analysis of REACT
- PMID: 30891808
- PMCID: PMC6461484
- DOI: 10.1111/apt.15214
Early combined immunosuppression may be effective and safe in older patients with Crohn's disease: post hoc analysis of REACT
Abstract
Background: Physicians may be reluctant to prescribe combined immunosuppression in older patients with Crohn's disease due to perceived risk of treatment-related complications.
Aim: To evaluate the impact of age on risk of Crohn's disease-related complications in patients treated with early combined immunosuppression vs conventional management in a post hoc analysis of the randomised evaluation of an algorithm for Crohn's treatment (REACT), a cluster-randomised trial.
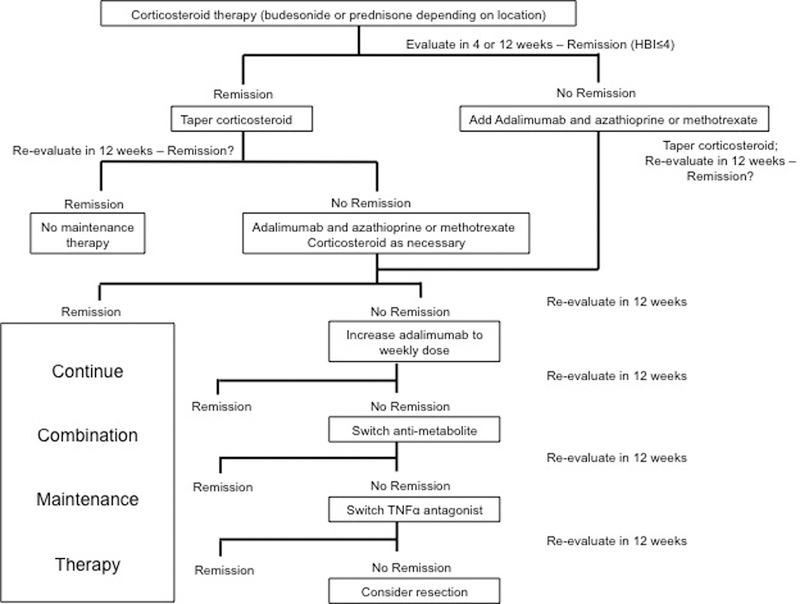
Methods: We compared efficacy (time to major adverse outcome of Crohn's disease-related surgery, hospitalisation or serious complications; corticosteroid-free clinical remission) and safety outcomes at 24 months, between patients aged <60 vs ≥60 years randomised to early combined immunosuppression or conventional management, using Cox proportional hazard analysis or modified Poisson model. In the early combined immunosuppression arm, patients with failure to achieve clinical remission within 4-12 weeks of corticosteroids were treated with a combination of tumour necrosis factor-α antagonist plus anti-metabolite and sequentially escalated in a stepwise algorithm.
Results: Of 1981 patients, 311 were ≥60 years (15.7%; 173 randomised to early combined immunosuppression and 138 to conventional management). Over 24 months, 10% of older patients developed Crohn's disease-related complications (early combined immunosuppression vs conventional management: 6.4% vs 14.5%) and 14 patients died (3.5% vs 5.8%). There was no difference between younger and older patients in risk of achieving corticosteroid-free clinical remission (<60 years, early combined immunosuppression (72.6%) vs conventional management (64.4%): relative risk [RR], 1.06 [95% CI, 0.98-1.15] vs ≥60 years, early combined immunosuppression (74.8%) vs conventional management (63.0%): RR, 1.09 [0.90-1.33], P-interaction = 0.78) or time to major adverse outcome (<60 years: hazard ratio [HR], 0.71 [0.53-0.96] vs ≥60 years: HR, 0.69 [0.31-1.51], P-interaction = 0.92) with early combined immunosuppression vs conventional management.
Conclusions: We observed no difference in efficacy and safety of early combined immunosuppression compared to conventional management in older and younger patients. Early combined immunosuppression may be considered as a treatment option in selected older patients with Crohn's disease with suboptimal disease control. Clinical Trial Identifier: NCT01030809.
© 2019 John Wiley & Sons Ltd.
Conflict of interest statement
Conflicts of Interest
Guangyong Zou: None
Figures
Comment in
-
Editorial: combination immunosuppressive therapy to treat Crohn's disease - ready for all age groups? Authors' reply.Aliment Pharmacol Ther. 2019 Jun;49(12):1529. doi: 10.1111/apt.15283. Aliment Pharmacol Ther. 2019. PMID: 31134649 Free PMC article. No abstract available.
-
Editorial: combination immunosuppressive therapy to treat Crohn's disease - ready for all age groups?Aliment Pharmacol Ther. 2019 Jun;49(12):1528. doi: 10.1111/apt.15259. Aliment Pharmacol Ther. 2019. PMID: 31134656 No abstract available.
-
Letter: immunogenicity of anti-TNF in elderly IBD patients-authors' reply.Aliment Pharmacol Ther. 2019 Aug;50(3):337. doi: 10.1111/apt.15379. Aliment Pharmacol Ther. 2019. PMID: 31313366 Free PMC article. No abstract available.
-
Letter: immunogenicity of anti-TNF in elderly IBD patients.Aliment Pharmacol Ther. 2019 Aug;50(3):336. doi: 10.1111/apt.15312. Aliment Pharmacol Ther. 2019. PMID: 31313368 No abstract available.
References
-
- Kaplan GG, Ng SC. Understanding and Preventing the Global Increase of Inflammatory Bowel Disease. Gastroenterology 2017;152(2):313–321 e2. - PubMed
-
- Dahlhamer JM, Zammitti EP, Ward BW, Wheaton AG, Croft JB. Prevalence of Inflammatory Bowel Disease Among Adults Aged >/=18 Years - United States, 2015. MMWR Morb Mortal Wkly Rep 2016;65(42):1166–1169. - PubMed
-
- Charpentier C, Salleron J, Savoye G, et al. Natural history of elderly-onset inflammatory bowel disease: a population-based cohort study. Gut 2014;63(3):423–32. - PubMed
-
- Heresbach D, Alexandre JL, Bretagne JF, et al. Crohn’s disease in the over-60 age group: a population based study. Eur J Gastroenterol Hepatol 2004;16(7):657–64. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical