

Prognostic Implication of Ventricular Conduction Disturbance Pattern in Hospitalized Patients with Acute Heart Failure Syndrome
- PMID: 30891964
- PMCID: PMC6597449
- DOI: 10.4070/kcj.2018.0290
Prognostic Implication of Ventricular Conduction Disturbance Pattern in Hospitalized Patients with Acute Heart Failure Syndrome
Abstract
Background and objectives: Conflicting data exist regarding the prognostic implication of ventricular conduction disturbance pattern in patients with heart failure (HF). This study investigated the prognostic impact of ventricular conduction pattern in hospitalized patients with acute HF.
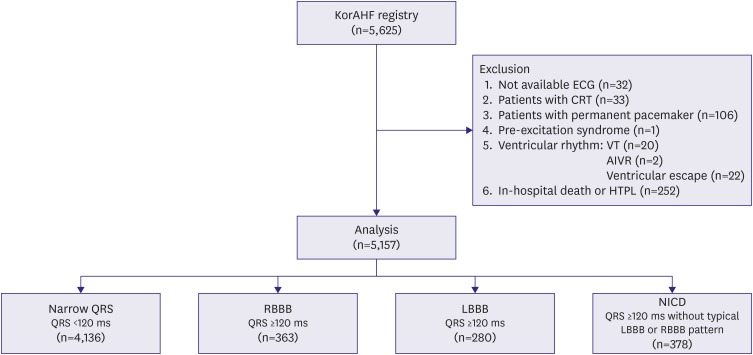
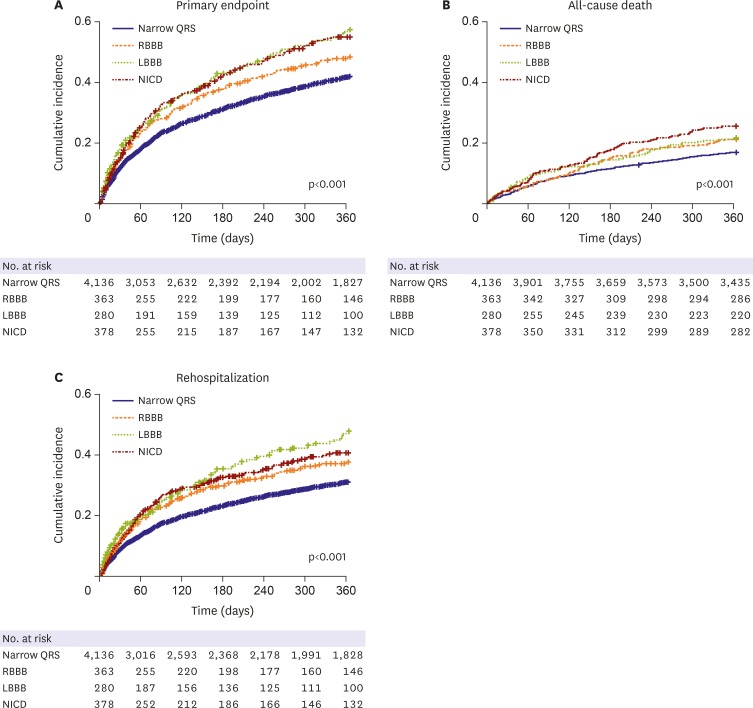
Methods: Data from the Korean Acute Heart Failure registry were used. Patients were categorized into four groups: narrow QRS (<120 ms), right bundle branch block (RBBB), left bundle branch block (LBBB), and nonspecific intraventricular conduction delay (NICD). The NICD was defined as prolonged QRS (≥120 ms) without typical features of LBBB or RBBB. The primary endpoint was the composite of all-cause mortality or rehospitalization for HF aggravation within 1 year after discharge.
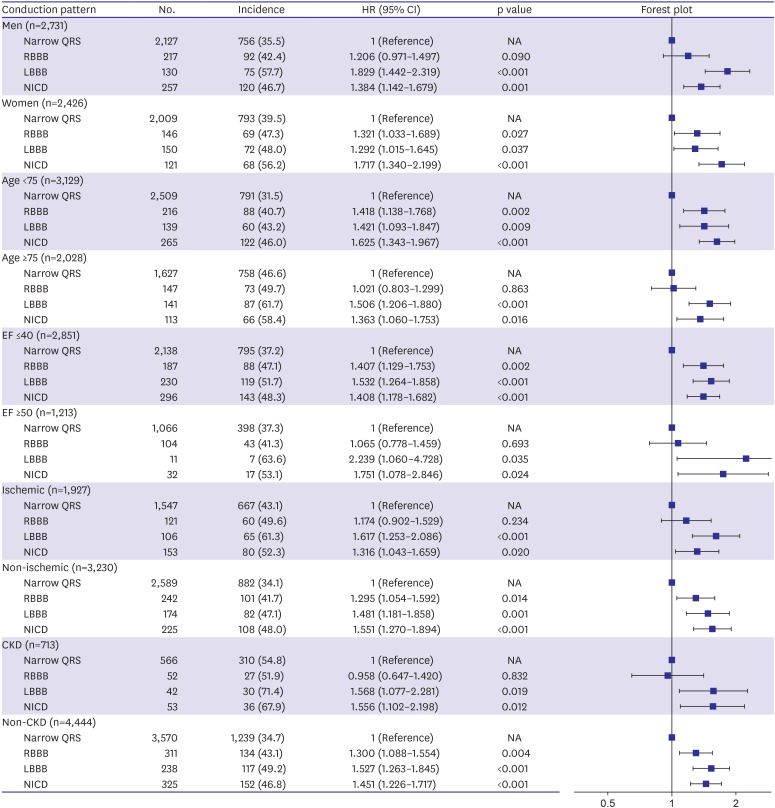
Results: This study included 5,157 patients. The primary endpoint occurred in 39.7% of study population. The LBBB group showed the highest incidence of primary endpoint followed by NICD, RBBB, and narrow QRS groups (52.5% vs. 49.7% vs. 44.4% vs. 37.5%, p<0.001). In a multivariable Cox-proportional hazards regression analysis, LBBB and NICD were associated with 39% and 28% increased risk for primary endpoint (LBBB hazard ratio [HR], 1.392; 95% confidence interval [CI], 1.152-1.681; NICD HR, 1.278; 95% CI, 1.074-1.520) compared with narrow QRS group. The HR of RBBB for the primary endpoint was 1.103 (95% CI, 0.915-1.329).
Conclusions: LBBB and NICD were independently associated with an increased risk of 1-year adverse event in hospitalized patients with HF, whereas the prognostic impacts of RBBB were limited.
Trial registration: ClinicalTrials.gov Identifier: NCT01389843.
Keywords: Bundle branch block; Cardiac conduction system disease; Heart failure; Prognosis.
Copyright © 2019. The Korean Society of Cardiology.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
Similar articles
-
The prognostic significance of bundle branch block in acute heart failure: a systematic review and meta-analysis.Clin Res Cardiol. 2023 Aug;112(8):1020-1043. doi: 10.1007/s00392-022-02105-z. Epub 2022 Sep 18. Clin Res Cardiol. 2023. PMID: 36116092
-
The Relationship of Conduction Disorder and Prognosis in Patients with Acute Coronary Syndrome.Int J Clin Pract. 2022 Oct 22;2022:9676434. doi: 10.1155/2022/9676434. eCollection 2022. Int J Clin Pract. 2022. PMID: 36340965 Free PMC article.
-
Cardiac Resynchronization Defibrillator Therapy for Nonspecific Intraventricular Conduction Delay Versus Right Bundle Branch Block.J Am Coll Cardiol. 2019 Jun 25;73(24):3082-3099. doi: 10.1016/j.jacc.2019.04.025. J Am Coll Cardiol. 2019. PMID: 31221257
-
Different patterns of bundle-branch blocks and the risk of incident heart failure in the Women's Health Initiative (WHI) study.Circ Heart Fail. 2013 Jul;6(4):655-61. doi: 10.1161/CIRCHEARTFAILURE.113.000217. Epub 2013 May 31. Circ Heart Fail. 2013. PMID: 23729198 Free PMC article.
-
Nonspecific intraventricular conduction delay: Definitions, prognosis, and implications for cardiac resynchronization therapy.Heart Rhythm. 2015 May;12(5):1071-9. doi: 10.1016/j.hrthm.2015.01.023. Epub 2015 Jan 19. Heart Rhythm. 2015. PMID: 25614250 Review.
Cited by
-
Paradigm Shifts of Heart Failure Therapy: Do We Need Another Paradigm?Int J Heart Fail. 2020 Apr 6;2(3):145-156. doi: 10.36628/ijhf.2020.0010. eCollection 2020 Jul. Int J Heart Fail. 2020. PMID: 36262366 Free PMC article. Review.
-
Artificial Intelligence-Based Electrocardiographic Biomarker for Outcome Prediction in Patients With Acute Heart Failure: Prospective Cohort Study.J Med Internet Res. 2024 Jul 3;26:e52139. doi: 10.2196/52139. J Med Internet Res. 2024. PMID: 38959500 Free PMC article.
-
The prognostic significance of bundle branch block in acute heart failure: a systematic review and meta-analysis.Clin Res Cardiol. 2023 Aug;112(8):1020-1043. doi: 10.1007/s00392-022-02105-z. Epub 2022 Sep 18. Clin Res Cardiol. 2023. PMID: 36116092
-
Deep learning of ECG waveforms for diagnosis of heart failure with a reduced left ventricular ejection fraction.Sci Rep. 2022 Aug 20;12(1):14235. doi: 10.1038/s41598-022-18640-8. Sci Rep. 2022. PMID: 35987961 Free PMC article.
-
Ventricular Conduction Disturbance in Acute Heart Failure Syndrome: Does It Matter for Prognosis?Korean Circ J. 2019 Jul;49(7):612-614. doi: 10.4070/kcj.2019.0116. Epub 2019 May 2. Korean Circ J. 2019. PMID: 31165596 Free PMC article. No abstract available.
References
-
- Wang NC, Maggioni AP, Konstam MA, et al. Clinical implications of QRS duration in patients hospitalized with worsening heart failure and reduced left ventricular ejection fraction. JAMA. 2008;299:2656–2666. - PubMed
-
- Mueller C, Laule-Kilian K, Klima T, et al. Right bundle branch block and long-term mortality in patients with acute congestive heart failure. J Intern Med. 2006;260:421–428. - PubMed
-
- Hong SJ, Oh J, Kang SM, et al. Clinical implication of right bundle branch block in hospitalized patients with acute heart failure: data from the Korean Heart Failure (KorHF) Registry. Int J Cardiol. 2012;157:416–418. - PubMed
-
- Abdel-Qadir HM, Tu JV, Austin PC, Wang JT, Lee DS. Bundle branch block patterns and long-term outcomes in heart failure. Int J Cardiol. 2011;146:213–218. - PubMed
Associated data
Grants and funding
- 2010-E63003-00/KCDC/Korea Centers for Disease Control & Prevention/Korea
- 2011-E63002-00/KCDC/Korea Centers for Disease Control & Prevention/Korea
- 2012-E63005-00/KCDC/Korea Centers for Disease Control & Prevention/Korea
- 2013-E63003-00/KCDC/Korea Centers for Disease Control & Prevention/Korea
- 2013-E63003-01/KCDC/Korea Centers for Disease Control & Prevention/Korea
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
