

ALK Resistance Mutations and Efficacy of Lorlatinib in Advanced Anaplastic Lymphoma Kinase-Positive Non-Small-Cell Lung Cancer
- PMID: 30892989
- PMCID: PMC6544460
- DOI: 10.1200/JCO.18.02236
ALK Resistance Mutations and Efficacy of Lorlatinib in Advanced Anaplastic Lymphoma Kinase-Positive Non-Small-Cell Lung Cancer
Abstract
Purpose: Lorlatinib is a potent, brain-penetrant, third-generation anaplastic lymphoma kinase (ALK)/ROS1 tyrosine kinase inhibitor (TKI) with robust clinical activity in advanced ALK-positive non-small-cell lung cancer, including in patients who have failed prior ALK TKIs. Molecular determinants of response to lorlatinib have not been established, but preclinical data suggest that ALK resistance mutations may represent a biomarker of response in previously treated patients.
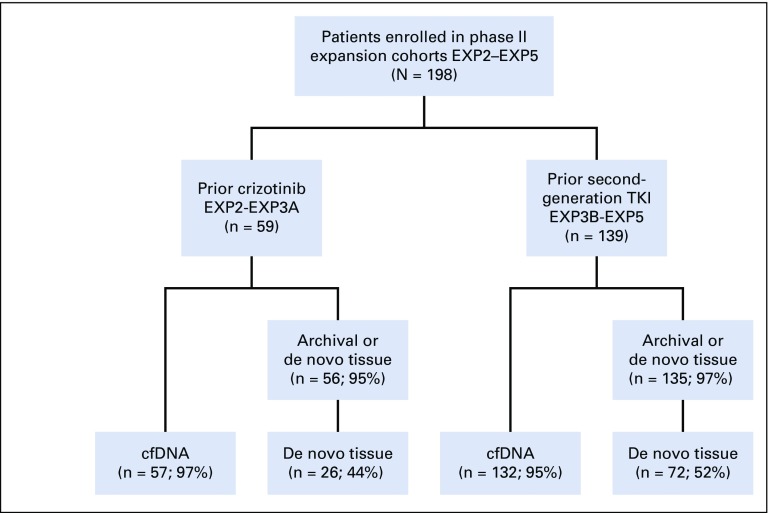
Patients and methods: Baseline plasma and tumor tissue samples were collected from 198 patients with ALK-positive non-small-cell lung cancer from the registrational phase II study of lorlatinib. We analyzed plasma DNA for ALK mutations using Guardant360. Tumor tissue DNA was analyzed using an ALK mutation-focused next-generation sequencing assay. Objective response rate, duration of response, and progression-free survival were evaluated according to ALK mutation status.
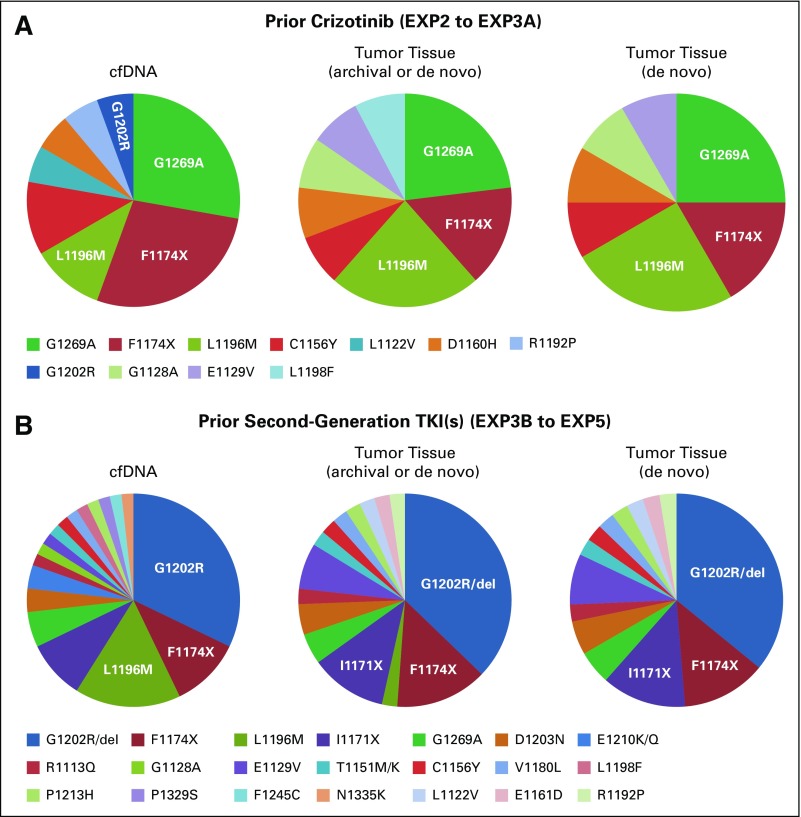
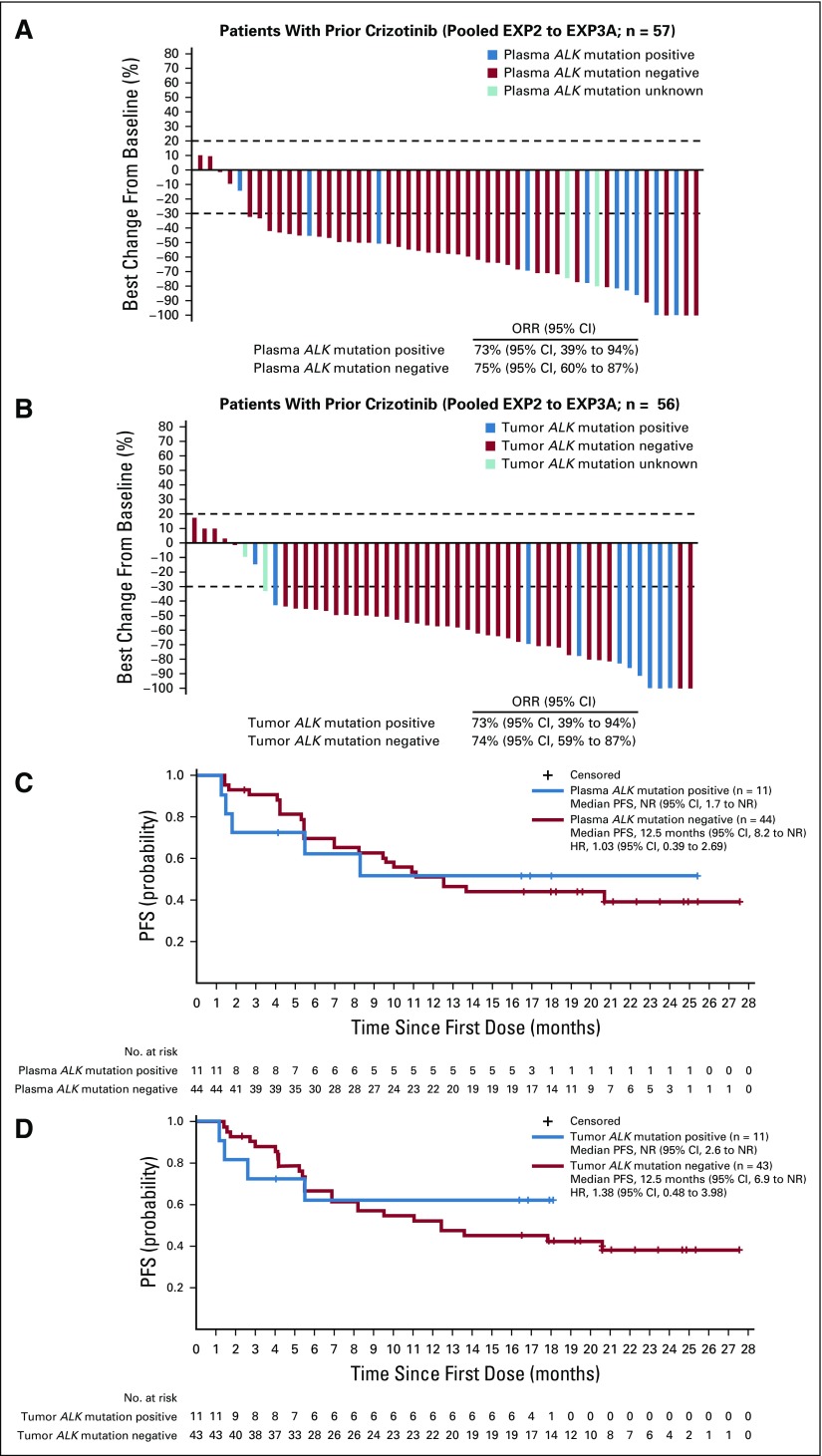
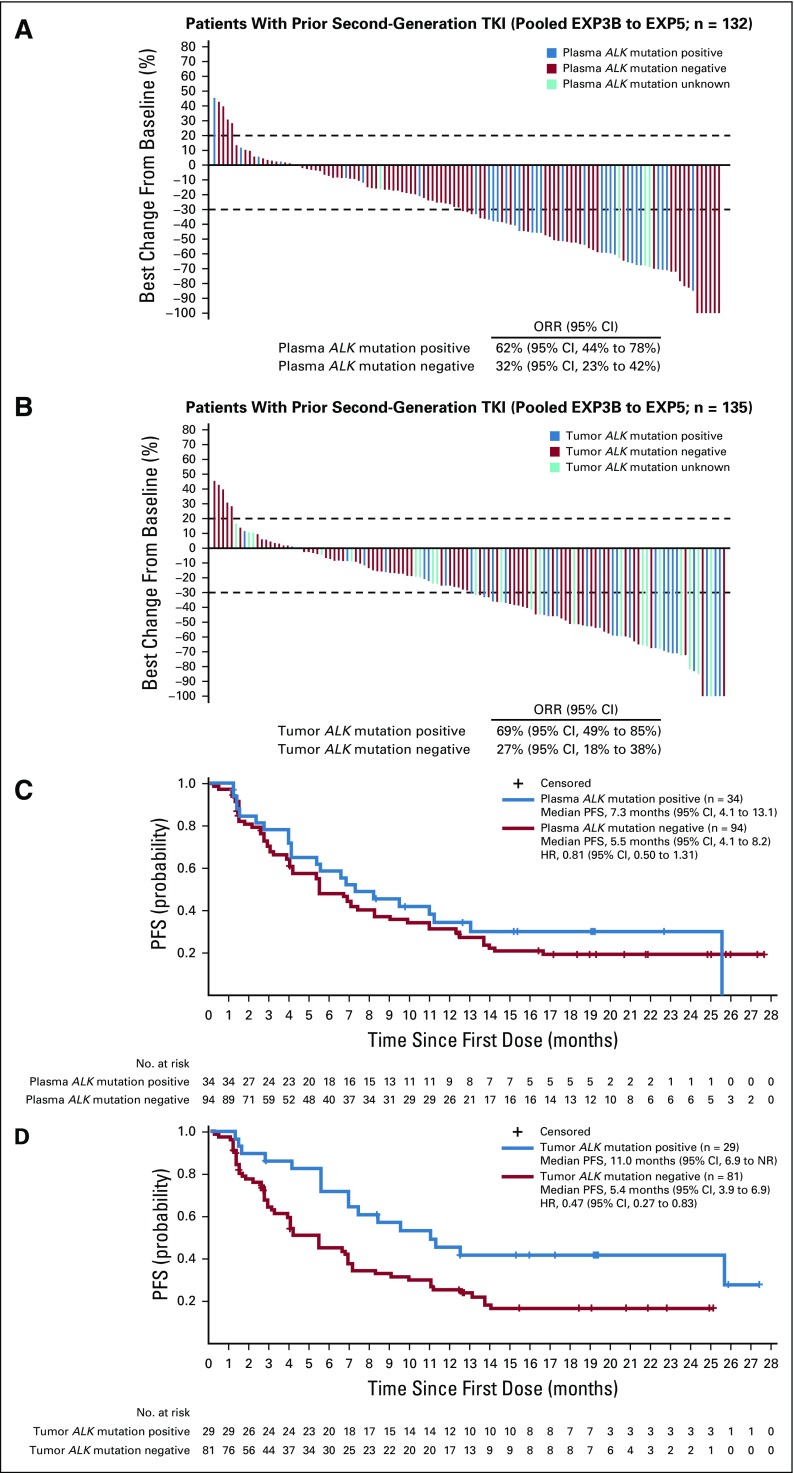
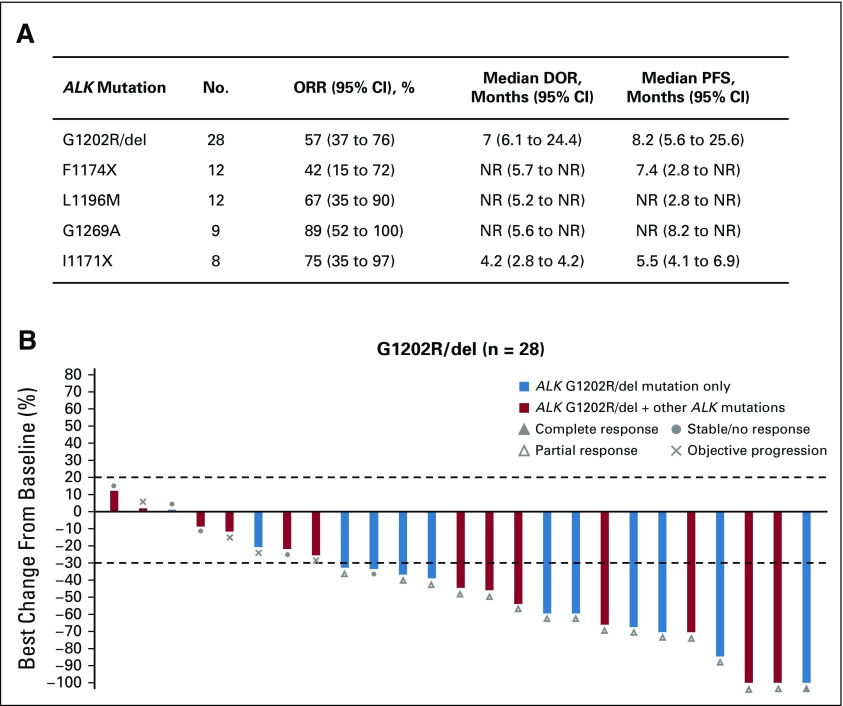
Results: Approximately one quarter of patients had ALK mutations detected by plasma or tissue genotyping. In patients with crizotinib-resistant disease, the efficacy of lorlatinib was comparable among patients with and without ALK mutations using plasma or tissue genotyping. In contrast, in patients who had failed 1 or more second-generation ALK TKIs, objective response rate was higher among patients with ALK mutations (62% v 32% [plasma]; 69% v 27% [tissue]). Progression-free survival was similar in patients with and without ALK mutations on the basis of plasma genotyping (median, 7.3 months v 5.5 months; hazard ratio, 0.81) but significantly longer in patients with ALK mutations identified by tissue genotyping (median, 11.0 months v 5.4 months; hazard ratio, 0.47).
Conclusion: In patients who have failed 1 or more second-generation ALK TKIs, lorlatinib shows greater efficacy in patients with ALK mutations compared with patients without ALK mutations. Tumor genotyping for ALK mutations after failure of a second-generation TKI may identify patients who are more likely to derive clinical benefit from lorlatinib.
Figures
Comment in
-
Stepping in the right direction but still some ways to go.Transl Cancer Res. 2019 Dec;8(Suppl 6):S603-S605. doi: 10.21037/tcr.2019.08.06. Transl Cancer Res. 2019. PMID: 35117141 Free PMC article. No abstract available.
References
-
- Soda M, Choi YL, Enomoto M, et al. Identification of the transforming EML4-ALK fusion gene in non–small-cell lung cancer. Nature. 2007;448:561–566. - PubMed
-
- Ou SH, Ahn JS, De Petris L, et al. Alectinib in crizotinib-refractory ALK-rearranged non–small-cell lung cancer: A phase II global study. J Clin Oncol. 2016;34:661–668. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
