

Association of PET-measured myocardial flow reserve with echocardiography-estimated pulmonary artery systolic pressure in patients with hypertrophic cardiomyopathy
- PMID: 30893304
- PMCID: PMC6426216
- DOI: 10.1371/journal.pone.0212573
Association of PET-measured myocardial flow reserve with echocardiography-estimated pulmonary artery systolic pressure in patients with hypertrophic cardiomyopathy
Abstract
Background: Pulmonary hypertension (PH) is a known complication of HCM and is a strong predictor of mortality. We aim to investigate the relationship between microvascular dysfunction measured by quantitative PET and PH in HCM patients.
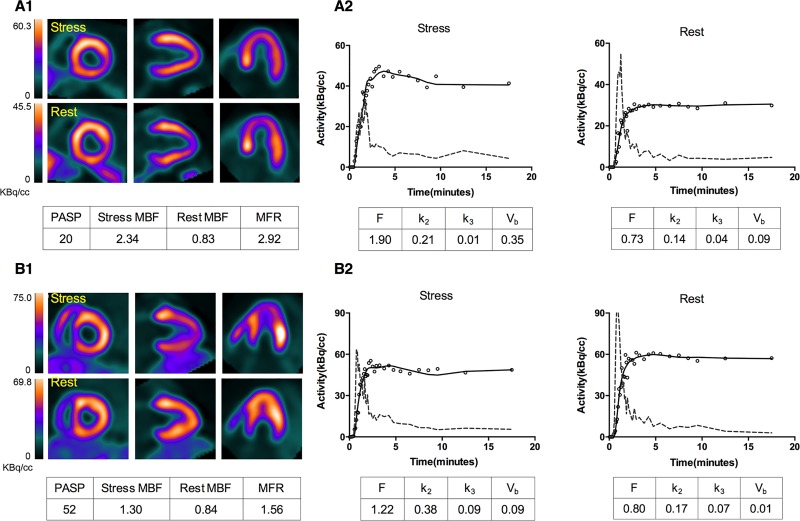
Methods: Eighty-nine symptomatic HCM patients were included in the study. Each patient underwent two 20-min 13N-NH3 dynamic PET scans for rest and stress conditions, respectively. A 2-tissue irreversible compartmental model was used to fit the segments time activity curves for estimating segmental and global myocardial blood flow (MBF) and myocardial flow reserve (MFR). Echocardiographic derived PASP was utilized to estimate PH.
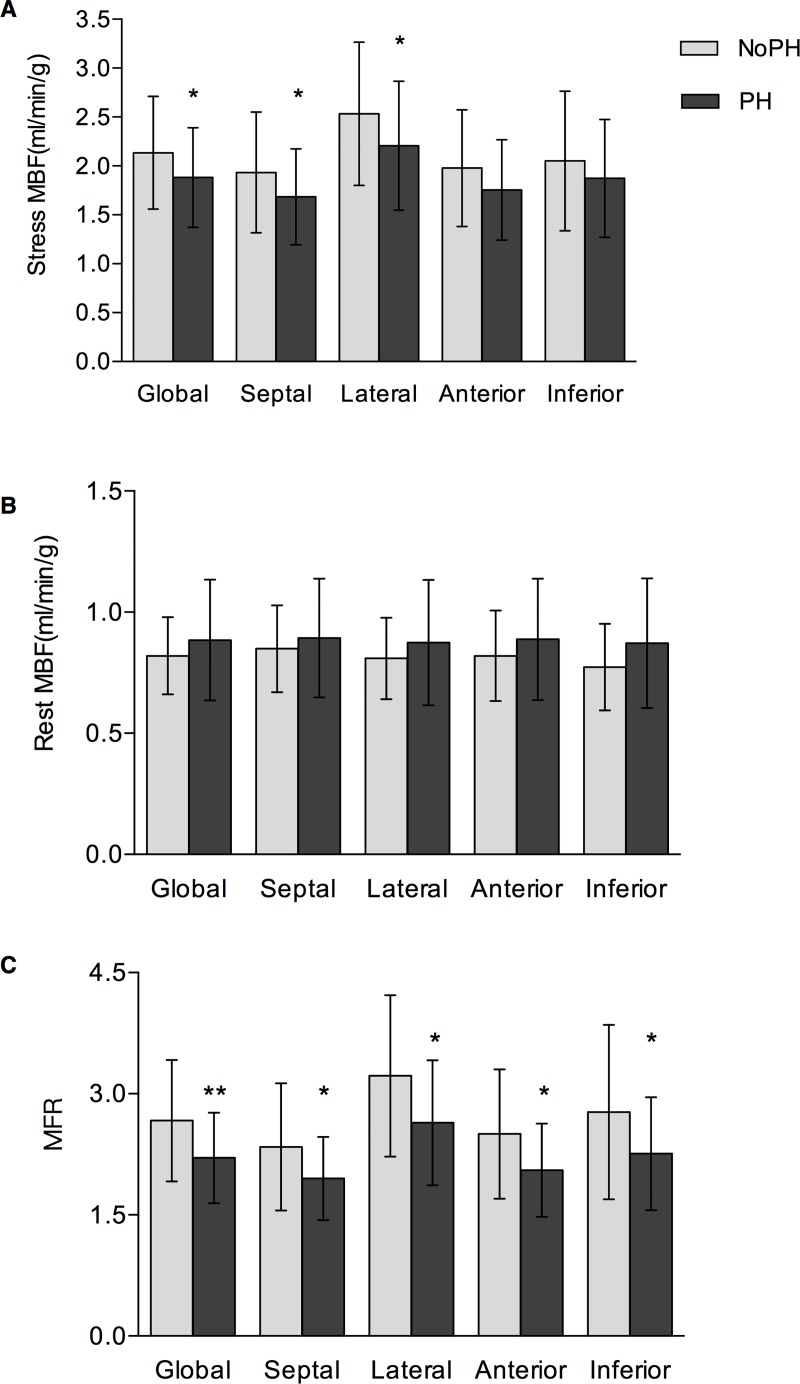
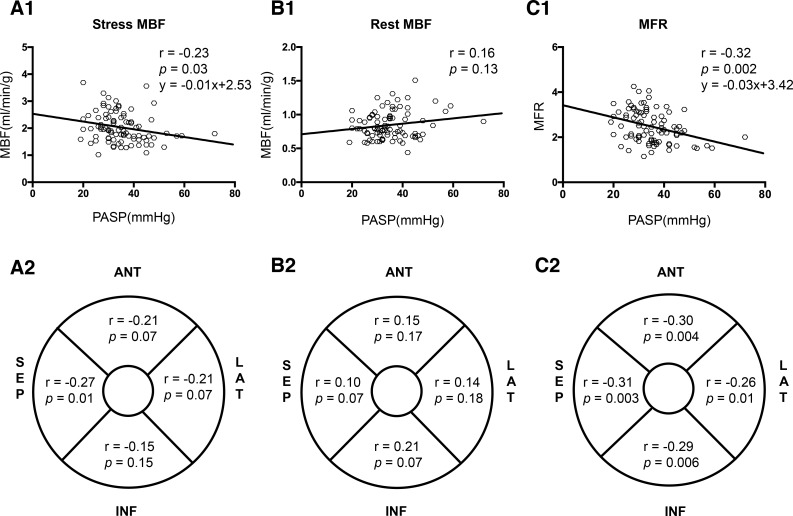
Results: Patients were categorized into two groups across PASP: PH (PASP > 36 mmHg) and no-PH (PASP ≤ 36 mmHg). patients with PH had larger left atrium, ratio of higher inflow early diastole (E) and atrial contraction (A) waves, E/A, and ratio of inflow and peak early diastolic waves, E/e', significantly reduced global stress MBF (1.85 ± 0.52 vs. 2.13 ± 0.56 ml/min/g; p = 0.024) and MFR (2.21 ± 0.57 vs. 2.62 ± 0.75; p = 0.005), while the MBFs at rest between the two groups were similar. There were significant negative correlations between global stress MBF/MFR and PASP (stress MBF: r = -0.23, p = 0.03; MFR: r = -0.32, p = 0.002); for regional MBF and MFR measurements, the highest linear correlation coefficients were observed in the septal wall (stress MBF: r = -0.27, p = 0.01; MFR: r = -0.31, p = 0.003). Global MFR was identified to be independent predictor for PH in multivariate regression analysis.
Conclusion: Echocardiography-derived PASP is negatively correlated with global MFR measured by 13N-NH3 dynamic PET. Global MFR is suggested to be an index of PH in HCM patients.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Comparison of two software systems for quantification of myocardial blood flow in patients with hypertrophic cardiomyopathy.J Nucl Cardiol. 2019 Aug;26(4):1243-1253. doi: 10.1007/s12350-017-1155-x. Epub 2018 Jan 22. J Nucl Cardiol. 2019. PMID: 29359273
-
Assessment of intravascular and extravascular mechanisms of myocardial perfusion abnormalities in obstructive hypertrophic cardiomyopathy by myocardial contrast echocardiography.Heart. 2007 Oct;93(10):1204-12. doi: 10.1136/hrt.2006.110460. Epub 2007 May 8. Heart. 2007. PMID: 17488767 Free PMC article.
-
Left ventricular diastolic inflow and myocardial flow reserve in patients with coronary artery disease: simultaneous analysis of 4D-Flow and myocardial perfusion using hybrid PETMR.Int J Cardiovasc Imaging. 2025 Jun;41(6):1075-1083. doi: 10.1007/s10554-025-03387-w. Epub 2025 Apr 10. Int J Cardiovasc Imaging. 2025. PMID: 40208431
-
Cardiac PET imaging for the detection and monitoring of coronary artery disease and microvascular health.JACC Cardiovasc Imaging. 2010 Jun;3(6):623-40. doi: 10.1016/j.jcmg.2010.04.007. JACC Cardiovasc Imaging. 2010. PMID: 20541718 Review.
-
Longitudinal myocardial blood flow gradient and CAD detection.Curr Cardiol Rep. 2015 Jan;17(1):550. doi: 10.1007/s11886-014-0550-z. Curr Cardiol Rep. 2015. PMID: 25417123 Review.
Cited by
-
The Utility of Nuclear Imaging in Hypertrophic Cardiomyopathy: A Narrative Review.J Clin Med. 2025 Mar 22;14(7):2183. doi: 10.3390/jcm14072183. J Clin Med. 2025. PMID: 40217634 Free PMC article. Review.
-
Microvascular Dysfunction as a Systemic Disease: A Review of the Evidence.Am J Med. 2022 Sep;135(9):1059-1068. doi: 10.1016/j.amjmed.2022.04.006. Epub 2022 Apr 23. Am J Med. 2022. PMID: 35472396 Free PMC article. Review.
References
-
- Gersh BJ, Maron BJ, Bonow RO, Dearani JA, Fifer MA, Link MS, et al. 2011 ACCF/AHA guideline for the diagnosis and treatment of hypertrophic cardiomyopathy: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2011;124(24):2761–96. 10.1161/CIR.0b013e318223e230 . - DOI - PubMed
-
- Authors/Task Force m, Elliott PM, Anastasakis A, Borger MA, Borggrefe M, Cecchi F, et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: the Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur Heart J. 2014;35(39):2733–79. 10.1093/eurheartj/ehu284 . - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
