

Group B Streptococcus early-onset disease and observation of well-appearing newborns
- PMID: 30893310
- PMCID: PMC6426194
- DOI: 10.1371/journal.pone.0212784
Group B Streptococcus early-onset disease and observation of well-appearing newborns
Abstract
Background: International guidelines lack a substantial consensus regarding management of asymptomatic full-term and late preterm neonates at risk for early-onset disease (EOS). Large cohorts of newborns are suitable to increase the understanding of the safety and efficacy of a given strategy.
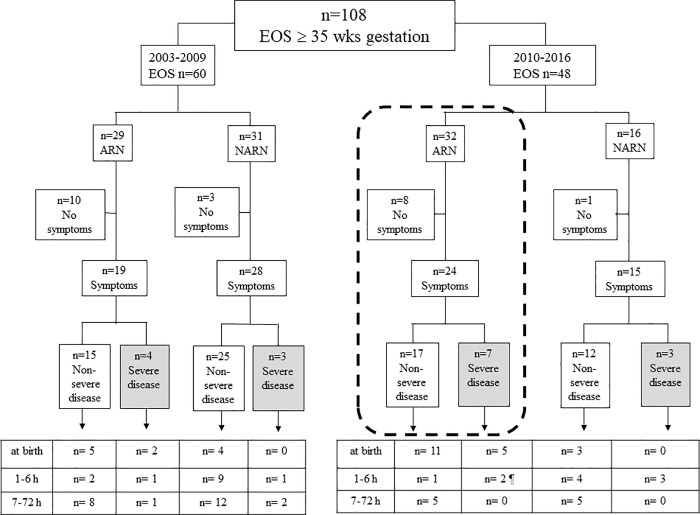
Methods: This is a prospective, area-based, cohort study involving regional birth facilities of Emilia-Romagna (Italy). We compared cases of EOS (at or above 35 weeks' gestation) registered in 2003-2009 (baseline period: 266,646 LBs) and in 2010-2016, after introduction of a new strategy (serial physical examinations, SPEs) for managing asymptomatic neonates at risk for EOS (intervention period: 265,508 LBs).
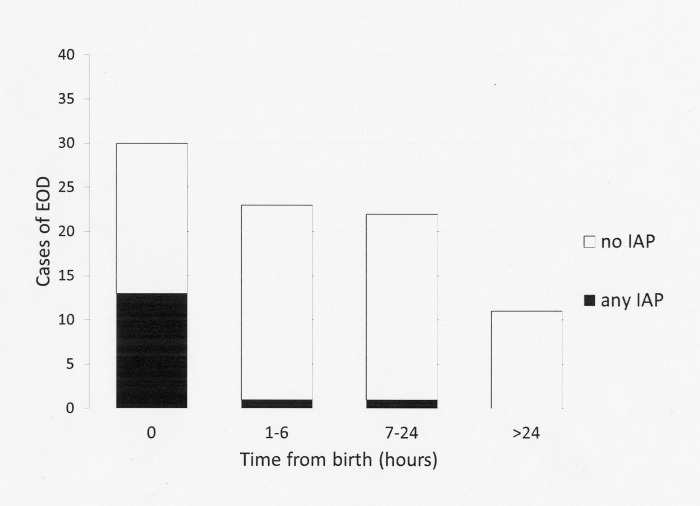
Results: There were 108 cases of EOS (baseline period, n = 60; intervention period, n = 48). Twenty-two (20.4%) remained asymptomatic through the first 72 hours of life, whereas 86 (79.6%) developed symptoms, in most cases (52/86, 60.5%) at birth or within 6 hours. The median age at presentation was significantly earlier in the intrapartum antibiotic prophylaxis (IAP)-exposed than in the IAP-unexposed neonates (0 hours, IQR 0.0000-0.0000 vs 6 hours, IQR 0.0000-15.0000, p<0.001). High number of neonates (n = 531) asymptomatic at birth, exposed to intrapartum fever, should be treated empirically for each newborn who subsequently develops sepsis. IAP exposed neonates increased (12% vs 33%, p = 0.01), age at presentation decreased (median 6 vs 1 hours, p = 0.01), whereas meningitis, mechanical ventilation and mortality did not change in baseline vs intervention period. After implementing the SPEs, no cases had adverse outcomes due to the strategy, and no cases developed severe disease after 6 hours of life.
Conclusions: Infants with EOS exposed to IAP developed symptoms at birth in almost all cases, and those who appeared well at birth had a very low chance of having EOS. The risk of EOS in neonates (asymptomatic at birth) exposed to intrapartum fever was low. Although definite conclusions on causation are lacking, our data support SPEs of asymptomatic newborns at risk for EOS. SPEs seems a safe and effective alternative to laboratory screening and empirical antibiotic therapy.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Verani JR, McGee L, Schrag SJ. Division of Bacterial Diseases, National Center for Immunization and Respiratory Diseases, Centres for Disease Control and Prevention (CDC). Prevention of perinatal group B streptococcal disease—revised guidelines from CDC, 2010. MMWR Recomm Rep 2010, 59 (RR-10):1–36 - PubMed
-
- Benitz WE, Gould JB, Druzin ML. Risk factors for early-onset group B streptococcal sepsis: estimation of odds ratios by critical literature review. Pediatrics. 1999;103:e77 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
