

Effectiveness of screening for atrial fibrillation and its determinants. A meta-analysis
- PMID: 30893323
- PMCID: PMC6426211
- DOI: 10.1371/journal.pone.0213198
Effectiveness of screening for atrial fibrillation and its determinants. A meta-analysis
Abstract
Background: Many atrial fibrillation patients eligible for oral anticoagulants are unaware of the presence of AF, and improved detection is necessary to facilitate thromboprophylaxis against stroke.
Objective: To assess the effectiveness of screening for AF compared to no screening and to compare efficacy outcomes of different screening strategies.
Materials and methods: Cochrane Central Register of Controlled Trials, EMBASE and MEDLINE from Jan 1, 2000 -Dec 31, 2015 were searched. Studies employing systematic or opportunistic screening and using ECG or pulse palpation in populations age ≥40 years were included. Data describing study and patient characteristics and number of patients with new AF were extracted. The outcome was the incidence of previously undiagnosed AF.
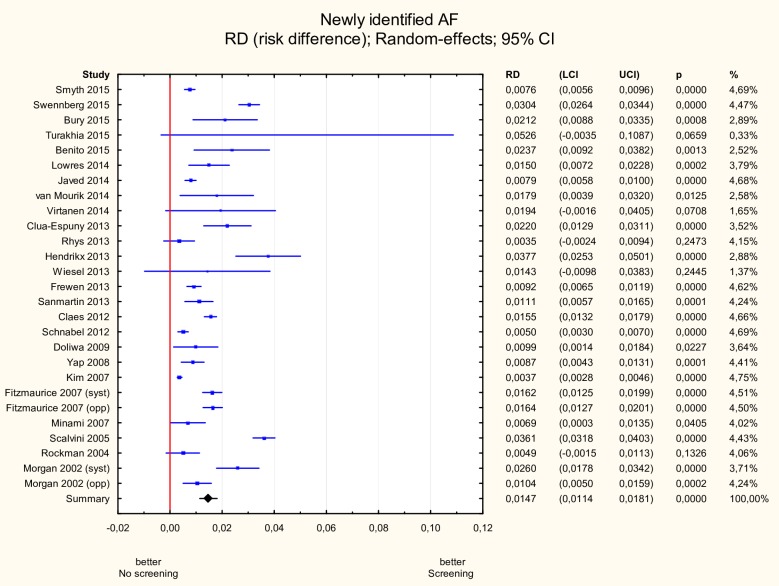
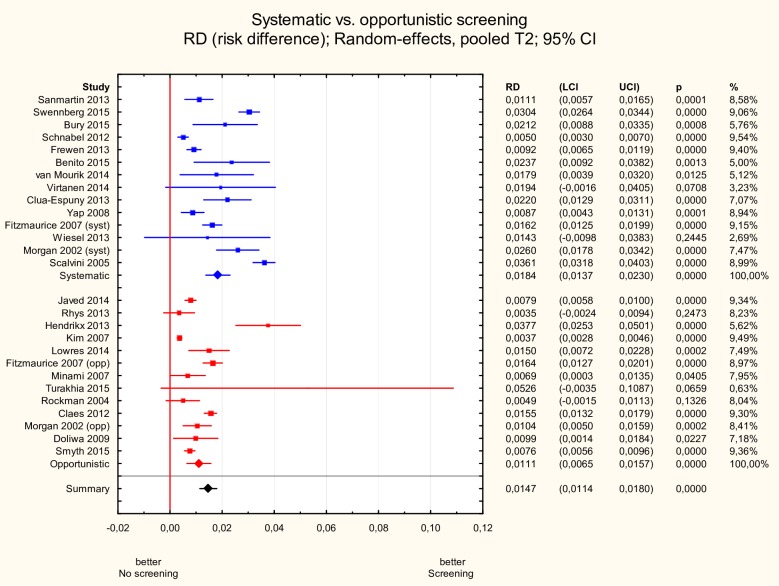
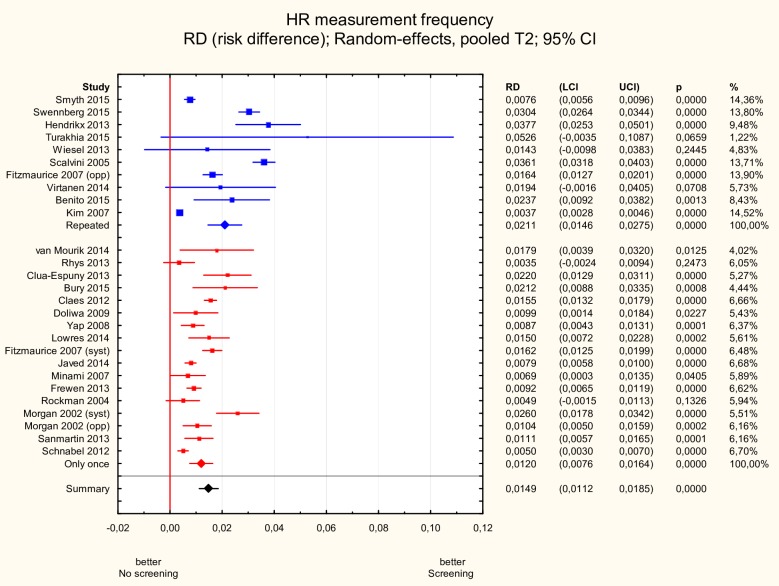
Results: We identified 25 unique (3 RCTs and 22 observational) studies (n = 88 786) from 14 countries. The incidence of newly detected AF due to screening was 1.5% (95% CI 1.1 to 1.8%). Systematic screening was more effective than opportunistic: 1.8% (95% CI 1.4 to 2.3%) vs. 1.1% (95% CI 0.6 to 1.6%), p<0.05, GP-led screening than community based: 1.9% (95% CI 1.4 to 2.4%) vs. 1.1% (95% CI 0.7 to 1.6%), p<0.05, and repeated heart rhythm measurements than isolated assessments of rhythm: 2.1% (95% CI 1.5-2.8) vs. 1.2% (95% CI 0.8-1.6), p<0.05. Only heart rhythm measurement frequency had statistical significance in a multivariate meta-regression model (p<0.05).
Conclusions: Active screening for AF, whether systematic or opportunistic, is effective beginning from 40 years of age. The organisation of screening process may be more important than technical solutions used for heart rhythm assessment.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures



References
-
- Miyasaka Y, Barnes ME, Gersh BJ, Cha SS, Bailey KR, Abhayaratna WP, et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation. 2006;114: 119–25. 10.1161/CIRCULATIONAHA.105.595140 - DOI - PubMed
-
- Chugh SS, Blackshear JL, Shen WK, Hammill SC, Gersh BJ. Epidemiology and natural history of atrial fibrillation: clinical implications. J Am Coll Cardiol. 2001;37: 371–8. - PubMed
-
- Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med. 2007;146: 857–67. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
