

Progressive parkinsonism in older adults is related to the burden of mixed brain pathologies
- PMID: 30894446
- PMCID: PMC6550497
- DOI: 10.1212/WNL.0000000000007315
Progressive parkinsonism in older adults is related to the burden of mixed brain pathologies
Abstract
Objective: To examine whether indices of Parkinson disease (PD) pathology and other brain pathologies are associated with the progression of parkinsonism in older adults.
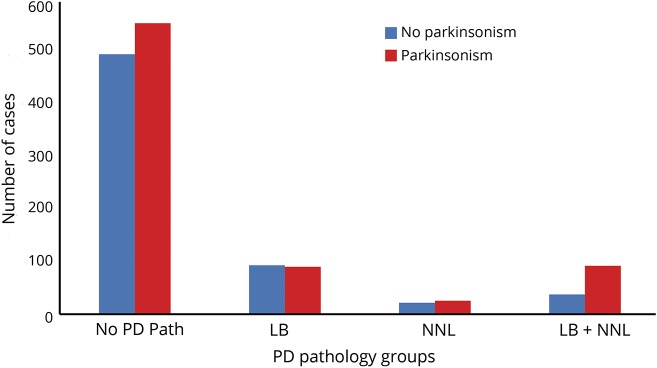
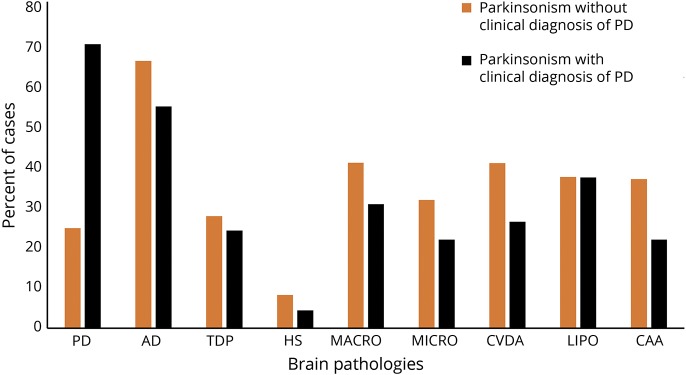
Methods: We used data from decedents who had undergone annual clinical testing prior to death and structured brain autopsy. Parkinsonism was based on assessment with a modified Unified Parkinson's Disease Rating Scale and a clinical diagnosis of PD was based on medical history. We used a series of mixed-effects models controlling for age and sex to investigate the association of PD pathology (nigral neuronal loss and Lewy bodies) and indices of 8 other brain pathologies with the progression of parkinsonism prior to death.
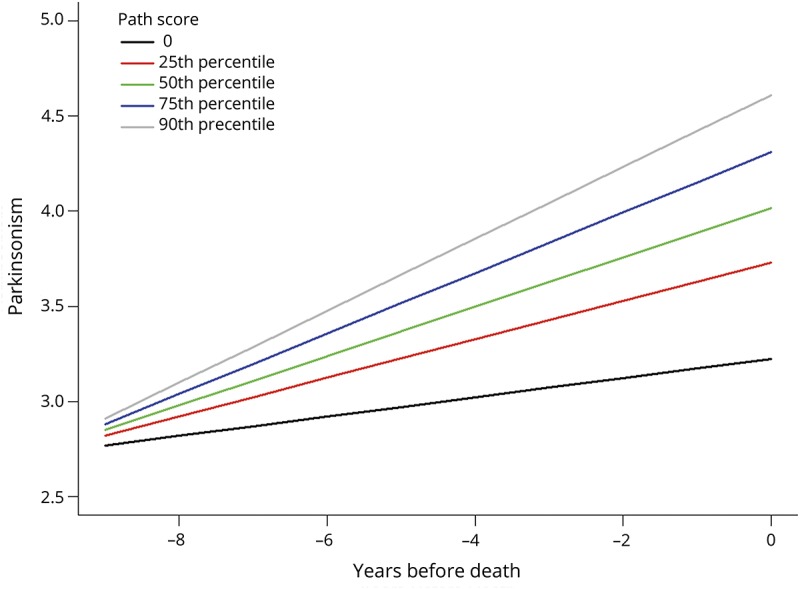
Results: During an average of 8.5 years' follow-up, more than half (771/1,430, 53.9%) developed parkinsonism proximate to death. On average, parkinsonism was progressive (estimate 0.130, SE 0.005, p < 0.001) in all older adults, but more rapid in adults with a clinical diagnosis of PD (n = 52; 3.6%) (estimate 0.066, SE 0.021, p < 0.001). Progression of parkinsonism was more rapid in adults with PD pathology (estimate 0.087, SE 0.013, p < 0.001). Alzheimer disease and several cerebrovascular pathologies were all independently associated with more rapid progression (all p values <0.05). The association between a higher person-specific weighted pathology score and more rapidly progressive parkinsonism did not differ between individuals with and without a clinical diagnosis of PD (estimate 0.003, SE 0.047, p = 0.957).
Conclusion: The rate of progressive parkinsonism in older adults with and without a clinical diagnosis of PD is related to the burden of mixed brain pathologies.
© 2019 American Academy of Neurology.
Figures
References
-
- Pringsheim T, Jette N, Frolkis A, Steeves TD. The prevalence of Parkinson's disease: a systematic review and meta-analysis. Mov Disord 2014;29:1583–1590. - PubMed
-
- Hofman A, de Jong PT, van Duijn CM, Breteler MM. Epidemiology of neurological diseases in elderly people: what did we learn from the Rotterdam Study? Lancet Neurol 2006;5:545–550. - PubMed
-
- Braak H, Tredici KD, Rüb U, de Vos RAI, Jansen Steur ENH, Braak E. Staging of brain pathology related to sporadic Parkinson's disease. Neurobiol Aging 2003;24:197–211. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources