

Delta-like protein 3 expression and therapeutic targeting in neuroendocrine prostate cancer
- PMID: 30894499
- PMCID: PMC6525633
- DOI: 10.1126/scitranslmed.aav0891
Delta-like protein 3 expression and therapeutic targeting in neuroendocrine prostate cancer
Abstract
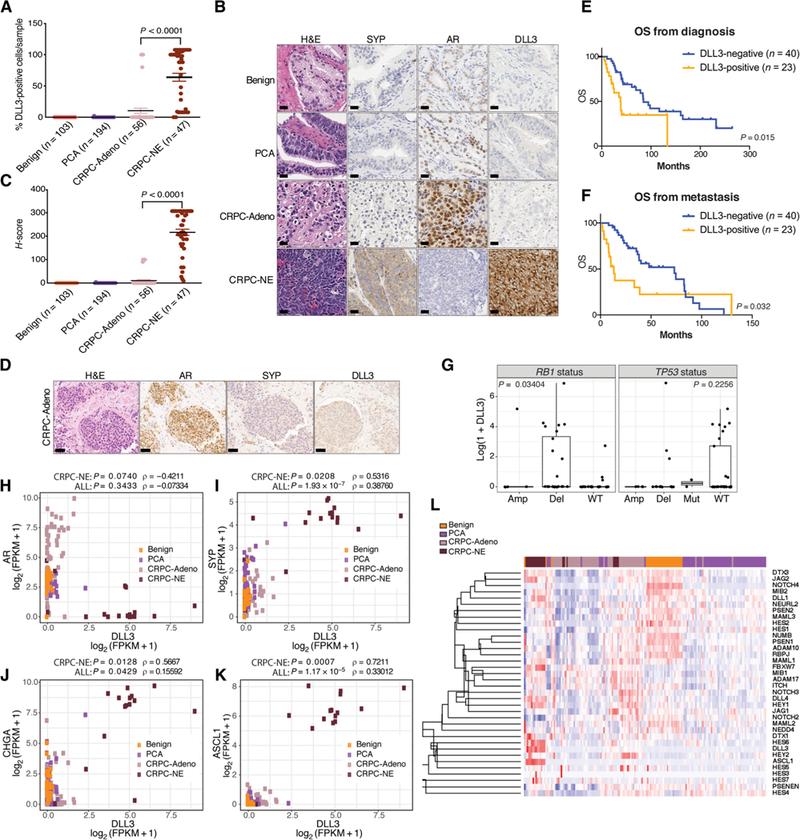
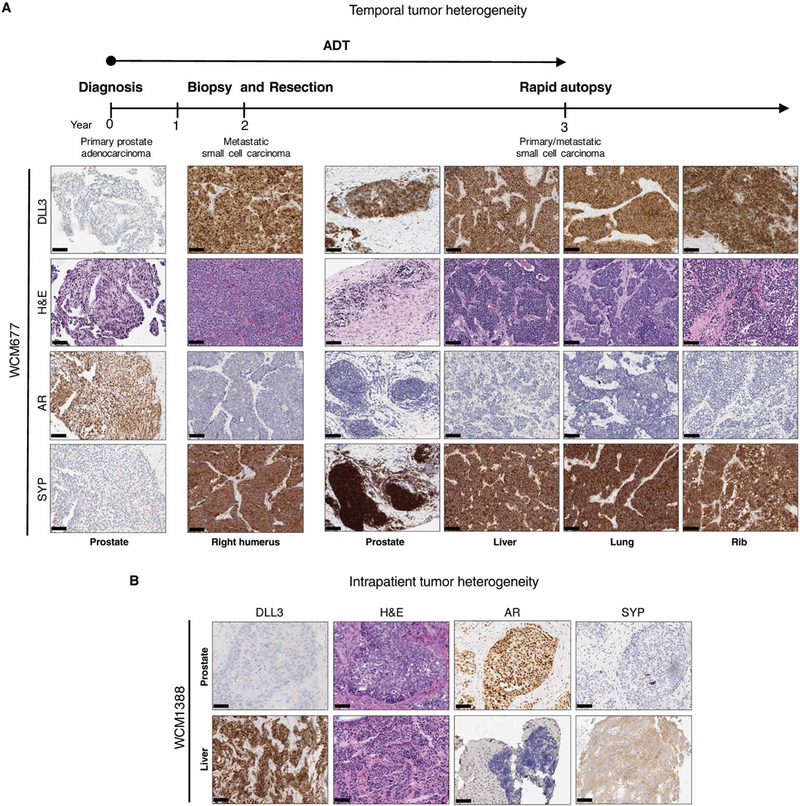
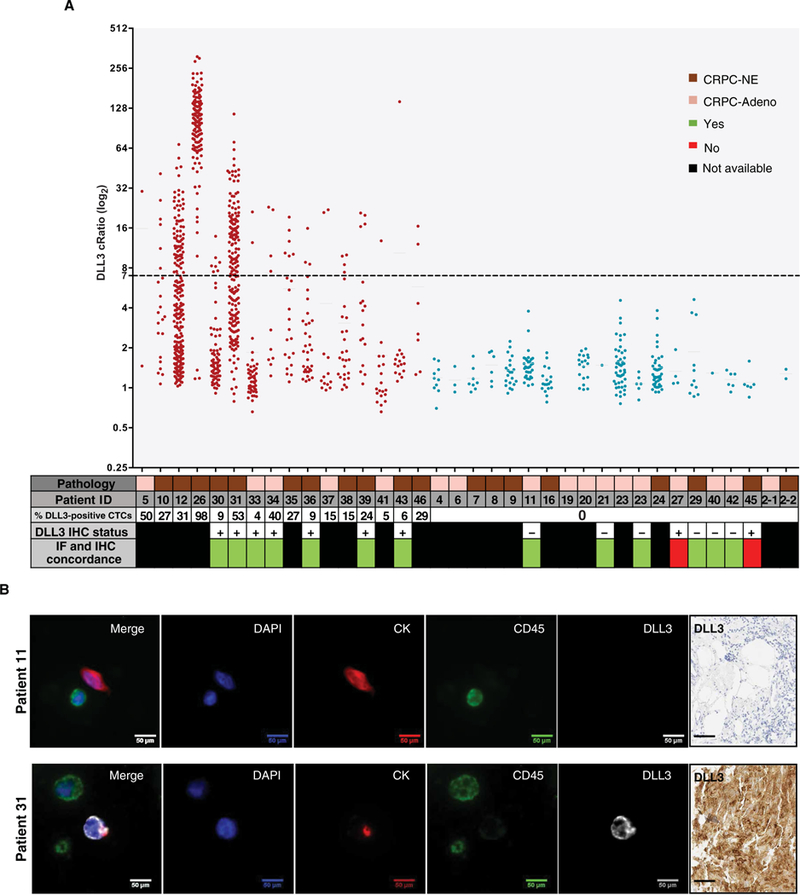
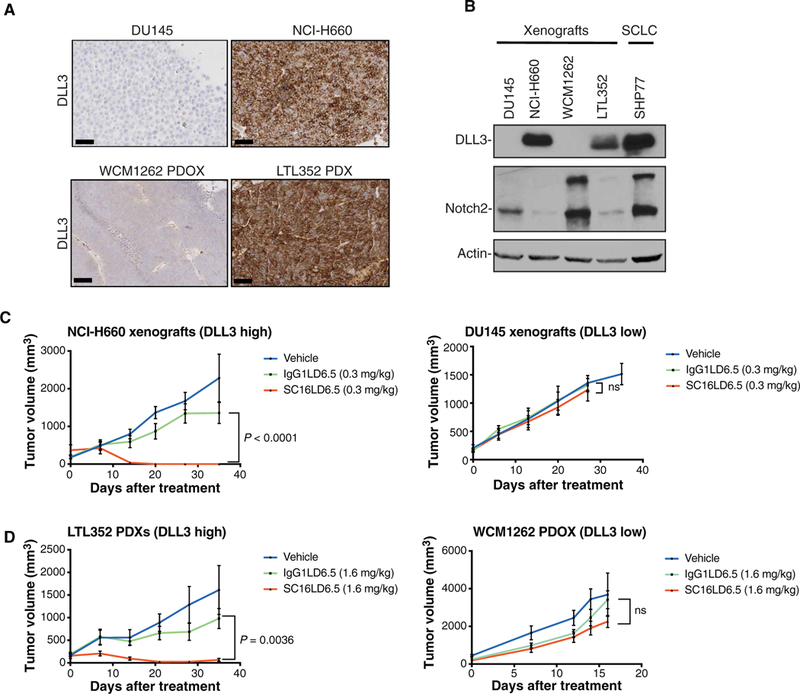
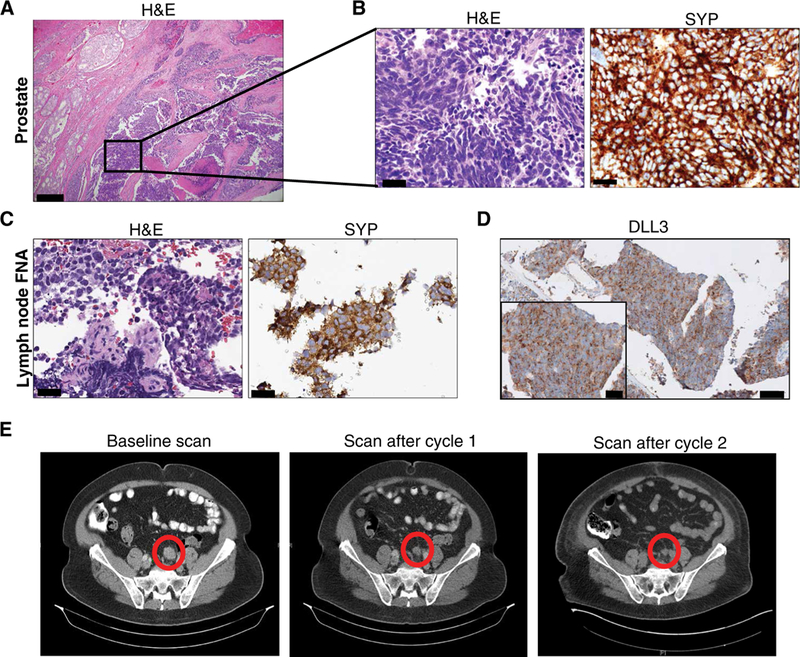
Histologic transformation to small cell neuroendocrine prostate cancer occurs in a subset of patients with advanced prostate cancer as a mechanism of treatment resistance. Rovalpituzumab tesirine (SC16LD6.5) is an antibody-drug conjugate that targets delta-like protein 3 (DLL3) and was initially developed for small cell lung cancer. We found that DLL3 is expressed in most of the castration-resistant neuroendocrine prostate cancer (CRPC-NE) (36 of 47, 76.6%) and in a subset of castration-resistant prostate adenocarcinomas (7 of 56, 12.5%). It shows minimal to no expression in localized prostate cancer (1 of 194) and benign prostate (0 of 103). DLL3 expression correlates with neuroendocrine marker expression, RB1 loss, and aggressive clinical features. DLL3 in circulating tumor cells was concordant with matched metastatic biopsy (87%). Treatment of DLL3-expressing prostate cancer xenografts with a single dose of SC16LD6.5 resulted in complete and durable responses, whereas DLL3-negative models were insensitive. We highlight a patient with neuroendocrine prostate cancer with a meaningful clinical and radiologic response to SC16LD6.5 when treated on a phase 1 trial. Overall, our findings indicate that DLL3 is preferentially expressed in CRPC-NE and provide rationale for targeting DLL3 in patients with DLL3-positive metastatic prostate cancer.
Copyright © 2019 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Conflict of interest statement
Figures
Comment in
-
Targeting DLL3 in neuroendocrine prostate cancer.Nat Rev Urol. 2019 Jun;16(6):330. doi: 10.1038/s41585-019-0190-6. Nat Rev Urol. 2019. PMID: 31040438 No abstract available.
References
-
- Beltran H, Rickman DS, Park K, Chae SS, Sboner A, MacDonald TY, Wang Y, Sheikh KL, Terry S, Tagawa ST, Dhir R, Nelson JB, de la Taille A, Allory Y, Gerstein MB, Perner S, Pienta KJ, Chinnaiyan AM, Wang Y, Collins CC, Gleave ME, Demichelis F, Nanus DM, Rubin MA, Molecular characterization of neuroendocrine prostate cancer and identification of new drug targets. Cancer Discov. 1, 487–495 (2011). - PMC - PubMed
-
- Beltran H, Prandi D, Mosquera JM, Benelli M, Puca L, Cyrta J, Marotz C, Giannopoulou E, Chakravarthi BVSK, Varambally S, Tomlins SA, Nanus DM, Tagawa ST, van Allen EM, Elemento O, Sboner A, Garraway LA, Rubin MA, Demichelis E, Divergent clonal evolution of castration-resistant neuroendocrine prostate cancer. Nat. Med. 22, 298–305 (2016). - PMC - PubMed
-
- Bluemn EG, Coleman IM, Lucas JM, Coleman RT, Hernandez-Lopez S, Tharakan R, Bianchi-Frias D, Dumpit RF, Kaipainen A, Corella AN, Yang YC, Nyquist MD, Mostaghel D, Hsieh AC, Zhang X, Corey E, Brown LG, Nguyen HM, Pienta K, Ittmann M, Schweizer M, True LD, Wise D, Rennie PS, Vessella RL, Morrissey C, Nelson PS, Androgen receptor pathway-independent prostate cancer is sustained through FGF signaling. Cancer Cell 32, 474–489.e6 (2017). - PMC - PubMed
-
- Aggarwal R, Huang J, Alumkal JJ, Zhang L, Feng FY, Thomas GV, Weinstein AS, Friedl V, Zhang C, Witte ON, Lloyd P, Gleave M, Evans CP, Youngren J, Beer TM, Rettig M, Wong CK, True L, Foye A, Playdle D, Ryan CJ, Lara P, Chi KN, Uzunangelov V, Sokolov A, Newton Y, Beltran H, Demichelis F, Rubin MA, Stuart JM, Small EJ, Clinical and genomic characterization of treatment-emergent small-cell neuroendocrine prostate cancer: A multi-institutional prospective study. J. Clin. Oncol. 36, 2492–2503 (2018). - PMC - PubMed
-
- Ku SY, Rosario S, Wang Y, Mu P, Seshadri M, Goodrich ZW, Goodrich MM, Labbé DP, Gomez EC, Wang J, Long HW, Xu B, Brown M, Loda M, Sawyers CL, Ellis L, Goodrich DW, Rb1 and Trp53 cooperate to suppress prostate cancer lineage plasticity, metastasis, and antiandrogen resistance. Science 355, 78–83 (2017). - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
