

Global Variation of Nutritional Status in Children Undergoing Chronic Peritoneal Dialysis: A Longitudinal Study of the International Pediatric Peritoneal Dialysis Network
- PMID: 30894599
- PMCID: PMC6426856
- DOI: 10.1038/s41598-018-36975-z
Global Variation of Nutritional Status in Children Undergoing Chronic Peritoneal Dialysis: A Longitudinal Study of the International Pediatric Peritoneal Dialysis Network
Abstract
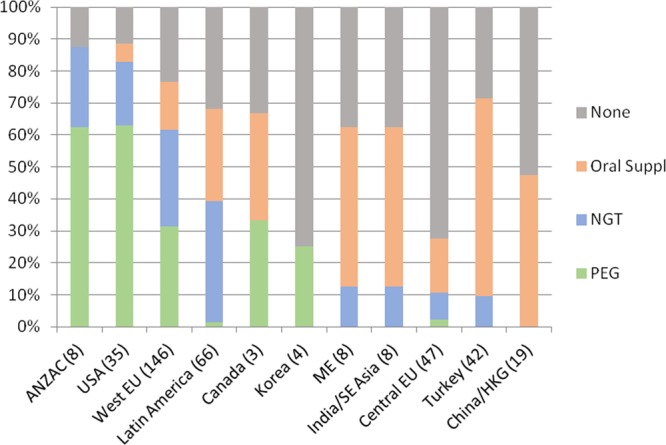
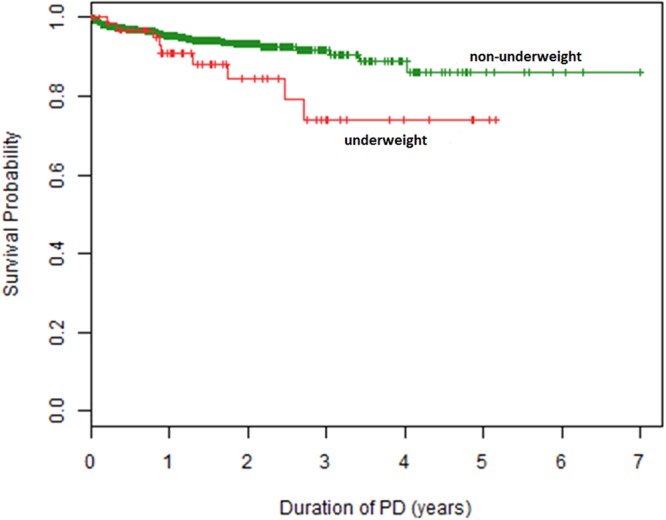
While children approaching end-stage kidney disease (ESKD) are considered at risk of uremic anorexia and underweight they are also exposed to the global obesity epidemic. We sought to investigate the variation of nutritional status in children undergoing chronic peritoneal dialysis (CPD) around the globe. The distribution and course of body mass index (BMI) standard deviation score over time was examined prospectively in 1001 children and adolescents from 35 countries starting CPD who were followed in the International Pediatric PD Network (IPPN) Registry. The overall prevalence of underweight, and overweight/obesity at start of CPD was 8.9% and 19.7%, respectively. Underweight was most prevalent in South and Southeast Asia (20%), Central Europe (16.7%) and Turkey (15.2%), whereas overweight and obesity were most common in the Middle East (40%) and the US (33%). BMI SDS at PD initiation was associated positively with current eGFR and gastrostomy feeding prior to PD start. Over the course of PD BMI SDS tended to increase on CPD in underweight and normal weight children, whereas it decreased in initially overweight patients. In infancy, mortality risk was amplified by obesity, whereas in older children mortality was markedly increased in association with underweight. Both underweight and overweight are prevalent in pediatric ESKD, with the prevalence varying across the globe. Late dialysis start is associated with underweight, while enteral feeding can lead to obesity. Nutritional abnormalities tend to attenuate with time on dialysis. Mortality risk appears increased with obesity in infants and with underweight in older children.
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Schaefer F, et al. IPPN investigators. Impact of global economic disparities on practices and outcomes of chronic peritoneal dialysis in children: insights from the International Pediatric Peritoneal Dialysis Network Registry. Perit Dial Int. 2012;32:399–409. doi: 10.3747/pdi.2012.00126. - DOI - PMC - PubMed
-
- WHO Multicentre Growth Reference Study Group WHO Child Growth Standards based on length/height, weight and age. Acta Paediatr Suppl. 2006;450:76–85. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
