Comparison of supine or prone crawl photon or proton breast and regional lymph node radiation therapy including the internal mammary chain
- PMID: 30894606
- PMCID: PMC6427000
- DOI: 10.1038/s41598-019-41283-1
Comparison of supine or prone crawl photon or proton breast and regional lymph node radiation therapy including the internal mammary chain
Abstract
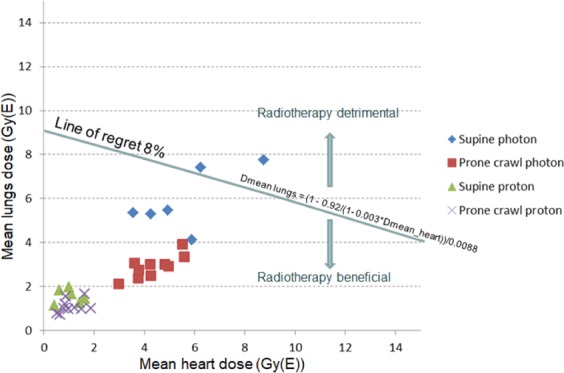
We report on a dosimetrical study comparing supine (S) and prone-crawl (P) position for radiotherapy of whole breast (WB) and loco-regional lymph node regions, including the internal mammary chain (LN_IM). Six left sided breast cancer patients were CT-simulated in S and P positions and four patients only in P position. Treatment plans were made using non-coplanar volumetric modulated arc photon therapy (VMAT) or pencil beam scanning intensity modulated proton therapy (IMPT). Dose prescription was 15*2.67 Gy(GyRBE). The average mean heart doses for S or P VMAT were 5.6 or 4.3 Gy, respectively (p = 0.16) and 1.02 or 1.08 GyRBE, respectively for IMPT (p = 0.8; p < 0.001 for IMPT versus VMAT). The average mean lung doses for S or P VMAT were 5.91 or 2.90 Gy, respectively (p = 0.002) and 1.56 or 1.09 GyRBE, respectively for IMPT (p = 0.016). In high-risk patients, average (range) thirty-year mortality rates from radiotherapy-related cardiac injury and lung cancer were estimated at 6.8(5.4-9.4)% or 3.8(2.8-5.1)% for S or P VMAT (p < 0.001), respectively, and 1.6(1.1-2.0)% or 1.2(0.8-1.6)% for S or P IMPT (p = 0.25), respectively. Radiation-related mortality risk could outweigh the ~8% disease-specific survival benefit of WB + LN_IM radiotherapy for S VMAT but not P VMAT. IMPT carries the lowest radiation-related mortality risks.
Conflict of interest statement
Ghent University is the applicant of the patent entitled Radiotherapy Board and Couch [WO2015144654A1] filed on 25.03.2014. Inventors are Wilfried De Neve, Bruno Speleers, Bert Boute and Liv Veldeman. Status of the patent: pending. The patent applies to the Prone Crawl Breast Couch used in this study.
Figures