

Altered Th17/Treg Ratio in Peripheral Blood of Systemic Lupus Erythematosus but Not Primary Antiphospholipid Syndrome
- PMID: 30894863
- PMCID: PMC6414457
- DOI: 10.3389/fimmu.2019.00391
Altered Th17/Treg Ratio in Peripheral Blood of Systemic Lupus Erythematosus but Not Primary Antiphospholipid Syndrome
Abstract
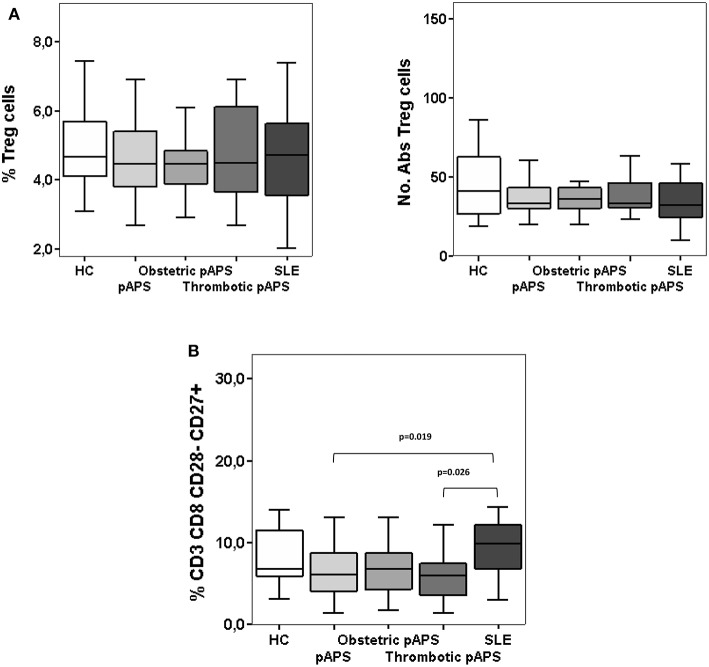
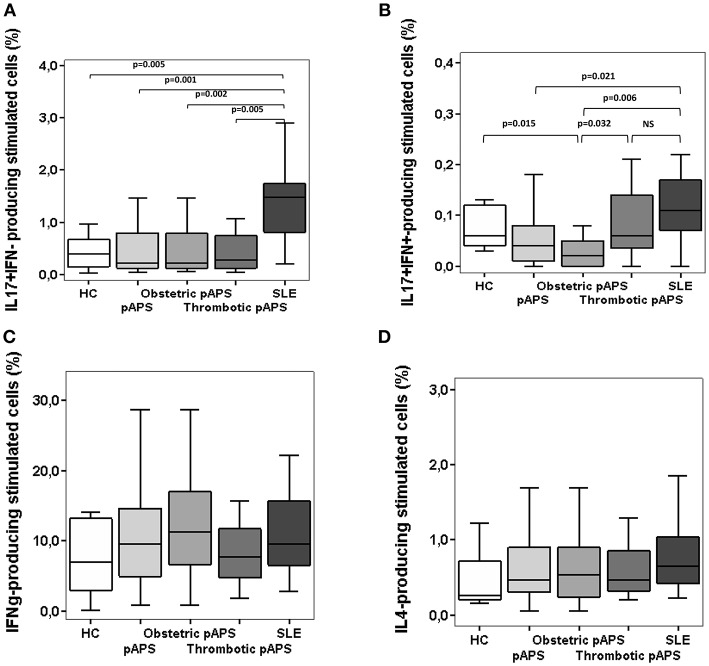
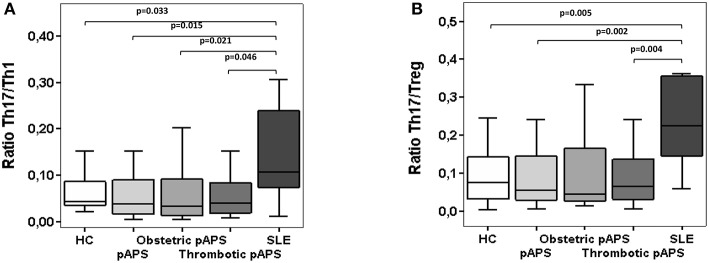
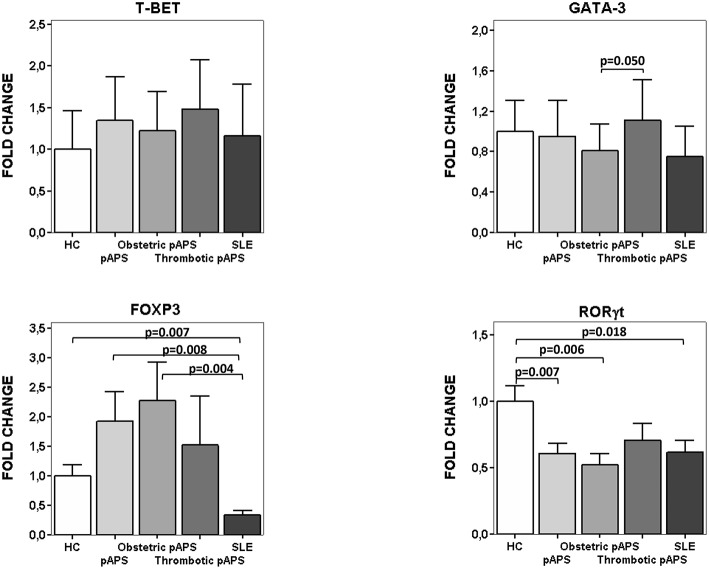
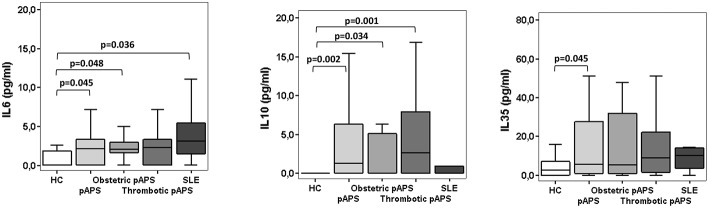
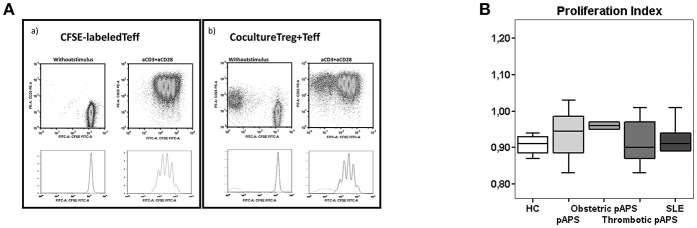
Introduction: The role of the immune response in the pathogenesis of antiphospholipid syndrome (APS) remains elusive. It is possible that differences in the frequencies of Th17 cells and/or defects in the immunoregulatory mechanisms are involved in the pathogenesis of APS. Our aim was to determine the peripheral blood Th cells phenotype and the circulating cytokine profile in patients with primary APS (pAPS) and compare it with systemic lupus erythemathosus (SLE) as disease control group. Methods: The frequencies of circulating regulatory T cells (Tregs) were determined in PBMCs from 36 patients with pAPS by flow cytometry. As control groups we included 21 age- and gender-matched healthy controls (HC) and 11 patients with SLE. The suppressive capacity of Tregs was evaluated in vitro by coculture assay. On the other hand, intracellular cytokine production was assessed in Th1, Th2, and Th17 cells and circulating IL-6, IL-10, and IL-35 were measured by Cytometric Bead Array and ELISA. The quantification of Th master gene expression levels was performed by real time quantitative PCR. Results: pAPS patients and SLE patients did not show differences in the percentage or number of Tregs compared to HC. The suppressive capacity of Tregs was also similar in the three study group. Instead, we found higher FoxP3·mRNA expression levels in pAPS patients and HC than SLE patients. Regarding the Th17 response, patients with pAPS and HC showed a significantly lower frequency of circulating Th17 cells than SLE. However, no differences were observed in the Th1 response between patients and controls. Thus, increased Th17/Th1 and Th17/Treg ratios were found in SLE patients but not in pAPS patients. pAPS and SLE patients had higher serum IL-6 levels than HC but there was not difference between both disease groups. Besides, a significant increase in the immunosuppressive cytokine levels was observed only in pAPS as compared to HC. Conclusions: Our data demonstrate an increased inflammatory profile of peripheral blood CD4+ T cells from SLE as compared with pAPS mostly due to an increased Th17 response. In conclusion, there seems not to be a direct pathogenic role for Th cells in pAPS but in SLE.
Keywords: SLE; Th1; Th17; Treg; inflammation; pAPS.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous