

Combining Radiation and Immune Checkpoint Blockade in the Treatment of Head and Neck Squamous Cell Carcinoma
- PMID: 30895168
- PMCID: PMC6414812
- DOI: 10.3389/fonc.2019.00122
Combining Radiation and Immune Checkpoint Blockade in the Treatment of Head and Neck Squamous Cell Carcinoma
Abstract
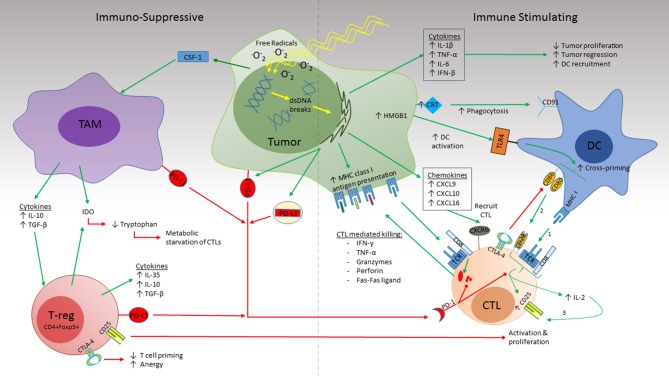
Head and neck squamous cell carcinoma (HNSCC) is a significant cause of morbidity and mortality worldwide. Current treatment options, even though potentially curative, have many limitations including a high rate of complications. Over the past few years immune checkpoint inhibitors (ICI) targeting cytotoxic lymphocyte antigen-4 (CTLA-4), programmed cell death protein 1 (PD-1), and programmed cell death ligand 1 (PD-L1) have changed treatment paradigms in many malignancies and are currently under investigation in HNSCC as well. Despite improvements in treatment outcomes and the implementation of combined modality approaches long-term survival rates in patients with locally advanced HNSCC remain suboptimal. Accumulating evidence suggests that under certain conditions, radiation may be delivered in conjunction with ICI to augment efficacy. In this review, we will discuss the immune modulating mechanisms of ICI and radiation, how changing the dose, fractionation, and field of radiation may alter the tumor microenvironment (TME), and how these two treatment modalities may work in concert to generate durable treatment responses against HNSCC.
Keywords: PD-L1; PD1; abscopal effect; immune checkpoint inhibitors; immunotherapy; radiation therapy.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous