

Cumulative live birth rates following a 'freeze-all' strategy: a population-based study
- PMID: 30895269
- PMCID: PMC6400239
- DOI: 10.1093/hropen/hoz004
Cumulative live birth rates following a 'freeze-all' strategy: a population-based study
Abstract
Study question: What is the cumulative live birth rate following a 'freeze-all' strategy compared with a 'fresh-transfer' strategy?
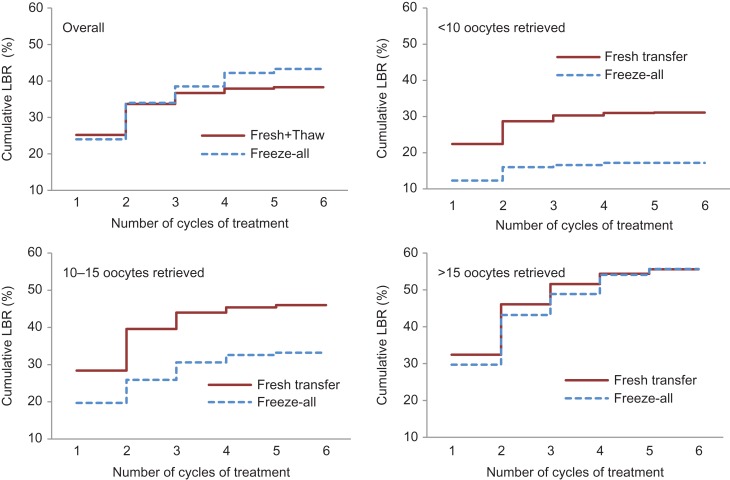
Summary answer: The 'freeze-all' strategy resulted in a similar cumulative live birth rate as the 'fresh-transfer' strategy among high responders (>15 oocytes retrieved) but did not benefit normal (10-15 oocytes) and suboptimal responders (<10 oocytes).
What is known already: Frozen-thawed embryo transfer is associated with a decreased risk of adverse obstetric and perinatal outcomes compared with fresh embryo transfer. It is unclear whether the 'freeze-all' strategy should be offered to all women undergoing ART treatment.
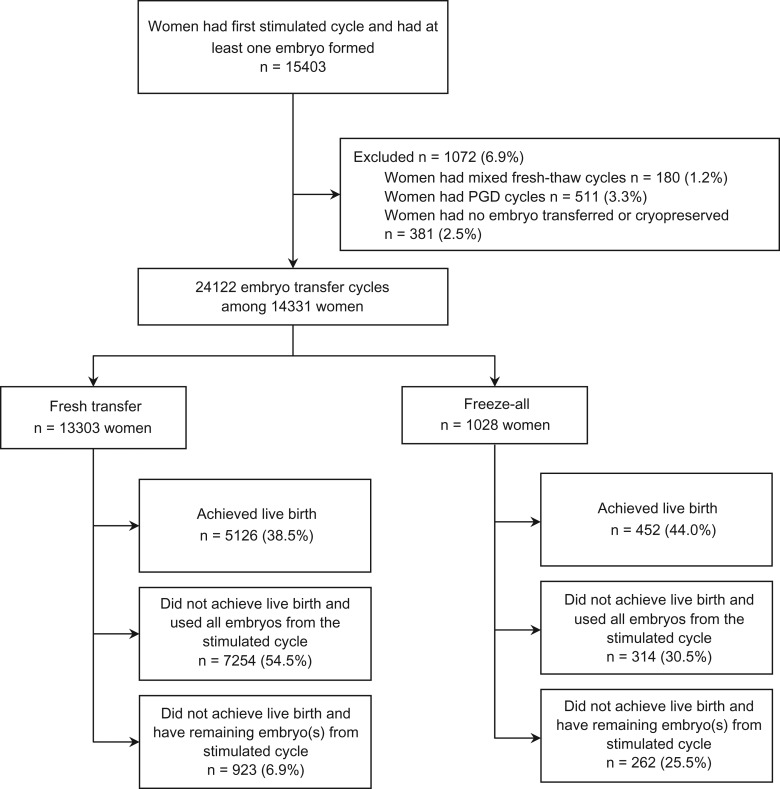
Study design size duration: A population-based retrospective cohort study using data collected by the Victorian Assisted Reproductive Treatment Authority. This study included 14 331 women undergoing their first stimulated ART cycle with at least one oocyte fertilised between 1 July 2009 and 30 June 2014 in Victoria, Australia. Demographic characteristics, type of ART procedures and resulting pregnancy and birth outcomes were recorded for the stimulated cycle and associated thaw cycles until 30 June 2016, or until a live birth was achieved, or until all embryos from the stimulated cycle had been used.
Participants/materials setting methods: Women were grouped by whether they had undergone the 'freeze-all' strategy (n = 1028) where all embryos were cryopreserved for future transfer, or the 'fresh-transfer' strategy (n = 13 303) where selected embryo(s) were transferred in the stimulated cycle, and remaining embryo(s) were cryopreserved for future use. A discrete-time survival model was used to evaluate the cumulative live birth rate following 'freeze-all' and 'fresh-transfer' strategy.
Main results and the role of chance: A total of 1028 women undergoing 'freeze-all' strategy and 13 303 women undergoing 'fresh-transfer' strategy had 1788 and 22 334 embryo transfer cycles resulting in 452 and 5126 live births, respectively. Most women (61.3%) in the 'freeze-all' group had more than 15 oocytes retrieved in the stimulated cycle compared with 18.1% of women in the 'fresh-transfer' group (P < 0.001). For high responders (>15 oocytes), the cumulative live birth rate in the 'freeze-all' group was similar to the 'fresh-transfer' group (56.8% vs. 56.2%, adjusted hazard ratio (AHR) 0.90, 95% CI 0.77-1.04). However, the likelihood of a live birth was lower in the 'freeze-all' group compared with the 'fresh-transfer' group among normal responders (10-15 oocytes) (33.2% vs. 46.3%, AHR 0.62, 95% CI 0.46-0.83) and suboptimal responders (<10 oocytes) (14.6% vs. 28.0%, AHR 0.67, 95% CI 0.14-1.01). During the minimum follow-up time of 2 years, 34.1%, 24.4% and 8.4% of suboptimal, normal and high responders, respectively, in the 'freeze-all' group did not return for any embryo transfer after the stimulated cycle, whereas all women in the 'fresh-transfer' group had at least one embryo transferred in the stimulated cycle.
Limitations reasons for caution: A limitation of this population-based study is the lack of information available on clinic-specific protocols for the 'freeze-all' strategy and the potential impact of these on outcomes. Data were not available on whether the 'freeze-all' strategy was used to prevent ovarian hyperstimulation syndrome (OHSS).
Wider implications of the findings: This study presents population-based evidence on clinical efficacy associated with a 'freeze-all' and 'fresh-transfer' strategy. The 'freeze-all' strategy may benefit some subgroups of patients, including women who are high responders and those who are at risk of OHSS, but should not be offered universally. Clinicians should consider the potential impact of electively deferring embryo transfer on treatment discontinuation in choosing the optimal embryo transfer strategy for couples undergoing ART treatment.
Study funding/competing interests: No specific funding was received to undertake this study. There is no conflict of interest, except that M.B. is a shareholder in Genea Ltd.
Keywords: ART; cryopreservation; cumulative rates; embryo transfer; freeze-only; live birth.
Figures
Similar articles
-
Cumulative live birth rates after one ART cycle including all subsequent frozen-thaw cycles in 1050 women: secondary outcome of an RCT comparing GnRH-antagonist and GnRH-agonist protocols.Hum Reprod. 2017 Mar 1;32(3):556-567. doi: 10.1093/humrep/dew358. Hum Reprod. 2017. PMID: 28130435 Clinical Trial.
-
Fresh versus frozen embryo transfers in assisted reproduction.Cochrane Database Syst Rev. 2021 Feb 4;2(2):CD011184. doi: 10.1002/14651858.CD011184.pub3. Cochrane Database Syst Rev. 2021. PMID: 33539543 Free PMC article.
-
ICSI does not increase the cumulative live birth rate in non-male factor infertility.Hum Reprod. 2018 Jul 1;33(7):1322-1330. doi: 10.1093/humrep/dey118. Hum Reprod. 2018. PMID: 29897449
-
Higher probability of live-birth in high, but not normal, responders after first frozen-embryo transfer in a freeze-only cycle strategy compared to fresh-embryo transfer: a meta-analysis.Hum Reprod. 2019 Mar 1;34(3):491-505. doi: 10.1093/humrep/dey388. Hum Reprod. 2019. PMID: 30689865
-
Conventional ovarian stimulation and single embryo transfer for IVF/ICSI. How many oocytes do we need to maximize cumulative live birth rates after utilization of all fresh and frozen embryos?Hum Reprod. 2016 Feb;31(2):370-6. doi: 10.1093/humrep/dev316. Epub 2016 Jan 2. Hum Reprod. 2016. PMID: 26724797
Cited by
-
Use of kisspeptin to trigger oocyte maturation during in vitro fertilisation (IVF) treatment.Front Endocrinol (Lausanne). 2022 Sep 6;13:972137. doi: 10.3389/fendo.2022.972137. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 36147569 Free PMC article. Review.
-
Good practice recommendations on add-ons in reproductive medicine†.Hum Reprod. 2023 Nov 2;38(11):2062-2104. doi: 10.1093/humrep/dead184. Hum Reprod. 2023. PMID: 37747409 Free PMC article.
-
Impact of elective frozen vs. fresh embryo transfer strategies on cumulative live birth: Do deleterious effects still exist in normal & hyper responders?PLoS One. 2020 Jun 26;15(6):e0234481. doi: 10.1371/journal.pone.0234481. eCollection 2020. PLoS One. 2020. PMID: 32589634 Free PMC article.
-
Study on the influence of syphilis on the outcome of frozen-thawed embryo transfer in infertility patients.Heliyon. 2024 Apr 6;10(8):e29342. doi: 10.1016/j.heliyon.2024.e29342. eCollection 2024 Apr 30. Heliyon. 2024. PMID: 38628734 Free PMC article.
-
Time associations between U.S. birth rates and add-Ons to IVF practice between 2005-2016.Reprod Biol Endocrinol. 2021 Jul 13;19(1):110. doi: 10.1186/s12958-021-00793-2. Reprod Biol Endocrinol. 2021. PMID: 34256798 Free PMC article.
References
-
- Acharya KS, Acharya CR, Bishop K, Harris B, Raburn D, Muasher SJ. Freezing of all embryos in in vitro fertilization is beneficial in high responders, but not intermediate and low responders: an analysis of 82,935 cycles from the Society for Assisted Reproductive Technology registry. Fertil Steril 2018;110:880–887. - PubMed
-
- Aflatoonian A, Mansoori-Torshizi M, Farid Mojtahedi M, Aflatoonian B, Khalili MA, Amir-Arjmand MH, Soleimani M, Aflatoonian N, Oskouian H, Tabibnejad N et al. . Fresh versus frozen embryo transfer after gonadotropin-releasing hormone agonist trigger in gonadotropin-releasing hormone antagonist cycles among high responder women: a randomized, multi-center study. Int J Reprod Biomed (Yazd) 2018;16:9–18. - PMC - PubMed
-
- Ata B, Seli E. A universal freeze all strategy: why it is not warranted. Curr Opin Obstet Gynecol 2017;29:136–145. - PubMed
-
- Blockeel C, Drakopoulos P, Santos-Ribeiro S, Polyzos NP, Tournaye H. A fresh look at the freeze-all protocol: a SWOT analysis. Hum Reprod 2016;31:491–497. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials