

Clinical outcomes and predictive model of platelet reactivity to clopidogrel after acute ischemic vascular events
- PMID: 30896564
- PMCID: PMC6595887
- DOI: 10.1097/CM9.0000000000000210
Clinical outcomes and predictive model of platelet reactivity to clopidogrel after acute ischemic vascular events
Abstract
Background: High on-treatment platelet reactivity (HTPR) has been suggested as a risk factor for patients with ischemic vascular disease. We explored a predictive model of platelet reactivity to clopidogrel and the relationship with clinical outcomes.
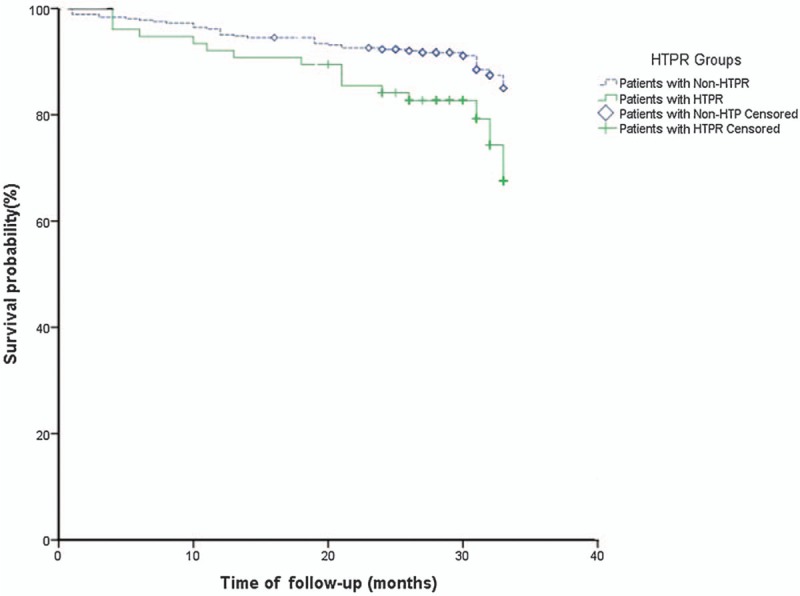
Methods: A total of 441 patients were included. Platelet reactivity was measured by light transmittance aggregometry after receiving dual antiplatelet therapy. HTPR was defined by the consensus cutoff of maximal platelet aggregation >46% by light transmittance aggregometry. CYP2C19 loss-of-function polymorphisms were identified by DNA microarray analysis. The data were compared by binary logistic regression to find the risk factors. The primary endpoint was major adverse clinical events (MACEs), and patients were followed for a median time of 29 months. Survival curves were constructed with Kaplan-Meier estimates and compared by log-rank tests between the patients with HTPR and non-HTPR.
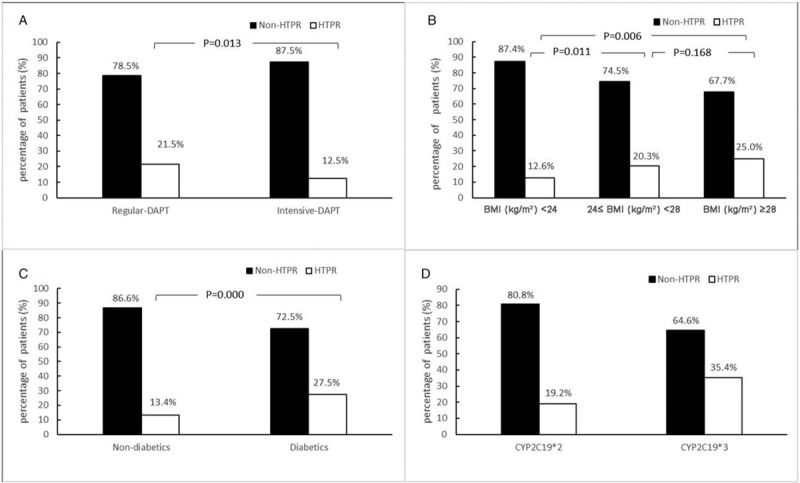
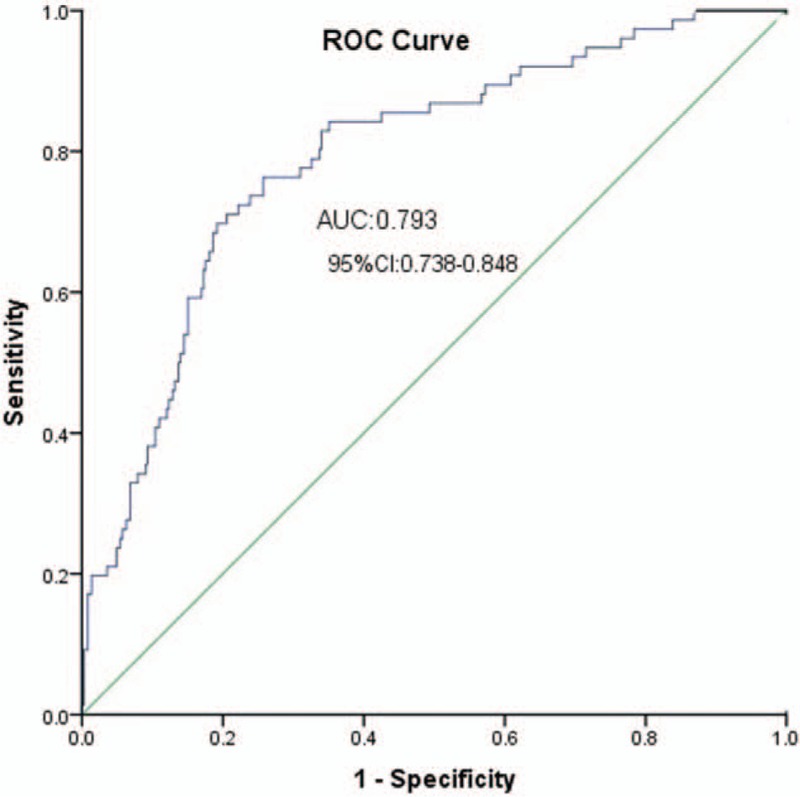
Results: The rate of HTPR was 17.2%. Logistic regression identified the following predictors of HTPR: age, therapy regimen, body mass index, diabetes history, CYP2C192, or CYP2C193 variant. The area under the curve of receiver operating characteristic for the HTPR predictive model was 0.793 (95% confidence interval: 0.738-0.848). Kaplan-Meier analysis showed that patients with HTPR had a higher incidence of MACE than those with non-HTPR (21.1% vs. 9.9%; χ = 7.572, P = 0.010).
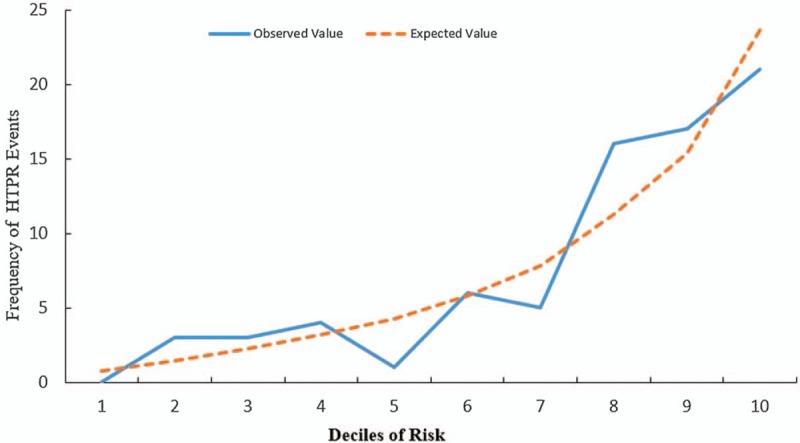
Conclusions: Our results suggest that advanced age, higher body mass index, treatment with regular dual antiplatelet therapy, diabetes, and CYP2C192 or CYP2C193 carriers are significantly associated with HTPR to clopidogrel. The predictive model of HTPR has useful discrimination and good calibration and may predict long-term MACE.
Figures
Similar articles
-
Pharmacodynamic effect of switching therapy in patients with high on-treatment platelet reactivity and genotype variation with high clopidogrel Dose versus prasugrel: the RESET GENE trial.Circ Cardiovasc Interv. 2012 Oct;5(5):698-704. doi: 10.1161/CIRCINTERVENTIONS.112.972463. Epub 2012 Oct 9. Circ Cardiovasc Interv. 2012. PMID: 23048056 Clinical Trial.
-
Association of clopidogrel high on-treatment reactivity with clinical outcomes and gene polymorphism in acute ischemic stroke patients: An observational study.Medicine (Baltimore). 2020 Apr;99(15):e19472. doi: 10.1097/MD.0000000000019472. Medicine (Baltimore). 2020. PMID: 32282698 Free PMC article.
-
The first in-human study to evaluate the antiplatelet properties of the clopidogrel conjugate DT-678 in acute coronary syndrome patients and healthy volunteers.Br J Pharmacol. 2025 Jan;182(1):131-141. doi: 10.1111/bph.17355. Epub 2024 Oct 4. Br J Pharmacol. 2025. PMID: 39367653 Clinical Trial.
-
High on-treatment platelet reactivity is associated with poor outcomes after ischemic stroke: A meta-analysis.Acta Neurol Scand. 2022 Sep;146(3):205-224. doi: 10.1111/ane.13655. Epub 2022 Jun 2. Acta Neurol Scand. 2022. PMID: 35652290 Review.
-
Platelet function/reactivity testing and prediction of risk of recurrent vascular events and outcomes after TIA or ischaemic stroke: systematic review and meta-analysis.J Neurol. 2020 Oct;267(10):3021-3037. doi: 10.1007/s00415-020-09932-y. Epub 2020 Jun 9. J Neurol. 2020. PMID: 32518978
Cited by
-
The Role of Genetic Polymorphism and Other Factors on Clopidogrel Resistance (CR) in an Asian Population with Coronary Heart Disease (CHD).Molecules. 2021 Apr 1;26(7):1987. doi: 10.3390/molecules26071987. Molecules. 2021. PMID: 33915807 Free PMC article. Review.
-
Identifying the Incidence, Predictors, Outcomes, and Prevention of Stent Thrombosis (ST) in Post-percutaneous Coronary Revascularization Patients With Drug-Eluting Stents (DES): A Systematic Review.Cureus. 2023 Sep 13;15(9):e45150. doi: 10.7759/cureus.45150. eCollection 2023 Sep. Cureus. 2023. PMID: 37842458 Free PMC article. Review.
-
The Novel Role of Noncoding RNAs in Modulating Platelet Function: Implications in Activation and Aggregation.Int J Mol Sci. 2023 Apr 21;24(8):7650. doi: 10.3390/ijms24087650. Int J Mol Sci. 2023. PMID: 37108819 Free PMC article. Review.
-
Impact of Acute Inflammation on Cytochromes P450 Activity Assessed by the Geneva Cocktail.Clin Pharmacol Ther. 2021 Jun;109(6):1668-1676. doi: 10.1002/cpt.2146. Epub 2021 Jan 8. Clin Pharmacol Ther. 2021. PMID: 33341941 Free PMC article.
-
METTL3-mediated methylation of CYP2C19 mRNA may aggravate clopidogrel resistance in ischemic stroke patients.Open Med (Wars). 2024 Feb 7;19(1):20240899. doi: 10.1515/med-2024-0899. eCollection 2024. Open Med (Wars). 2024. PMID: 38463525 Free PMC article.
References
-
- Wang W, Jiang B, Sun H, Ru X, Sun D, Wang L, et al. Prevalence, incidence, and mortality of stroke in China: results from a nationwide population-based survey of 480 687 adults. Circulation 2017; 135:759–771. doi: 10.1161/CIRCULATIONAHA.116.025250. - PubMed
-
- Murray CJ, Lopez AD. Measuring the global burden of disease. N Engl J Med 2013; 369:448–457. doi: 10.1056/NEJMra1201534. - PubMed
-
- Liu M, Wu B, Wang WZ, Lee LM, Zhang SH, Kong LZ. Stroke in China: epidemiology, prevention, and management strategies. Lancet Neurol 2007; 6:456–464. doi: 10.1016/S1474-4422(07)70004-2. - PubMed
-
- Kiernan TJ, Yan BP, Jaff MR. Antiplatelet therapy for the primary and secondary prevention of cerebrovascular events in patients with extracranial carotid artery disease. J Vasc Surg 2009; 50:431–439. doi: 10.1016/j.jvs.2009.04.052. - PubMed
-
- Xu H, Ping Y, Lin H, He P, Li W, Dai H. Antiplatelet strategies and outcomes in patients with noncardioembolic ischemic stroke from a real-world study with a five-year follow-up. Transl Stroke Res 2017; 8:228–233. doi: 10.1007/s12975-016-0516-0. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
