

Continuous blood purification for severe acute pancreatitis: A systematic review and meta-analysis
- PMID: 30896634
- PMCID: PMC6708963
- DOI: 10.1097/MD.0000000000014873
Continuous blood purification for severe acute pancreatitis: A systematic review and meta-analysis
Abstract
Background: The incidence of acute pancreatitis (AP) is rising around the world, thus further increasing the burden on healthcare services. Approximately 20% of AP will develop severe acute pancreatitis (SAP) with persistent organ failure (>48 h), which is the leading cause of high mortality. To date, there is no specific drug in treating SAP, and the main treatment is still based on supportive care. However, some clinical control studies regarding the superiority of continuous blood purification (CBP) has been published recently. Therefore, we conducted a systematic review and meta-analysis to evaluate the efficacy of CBP in SAP treatment.
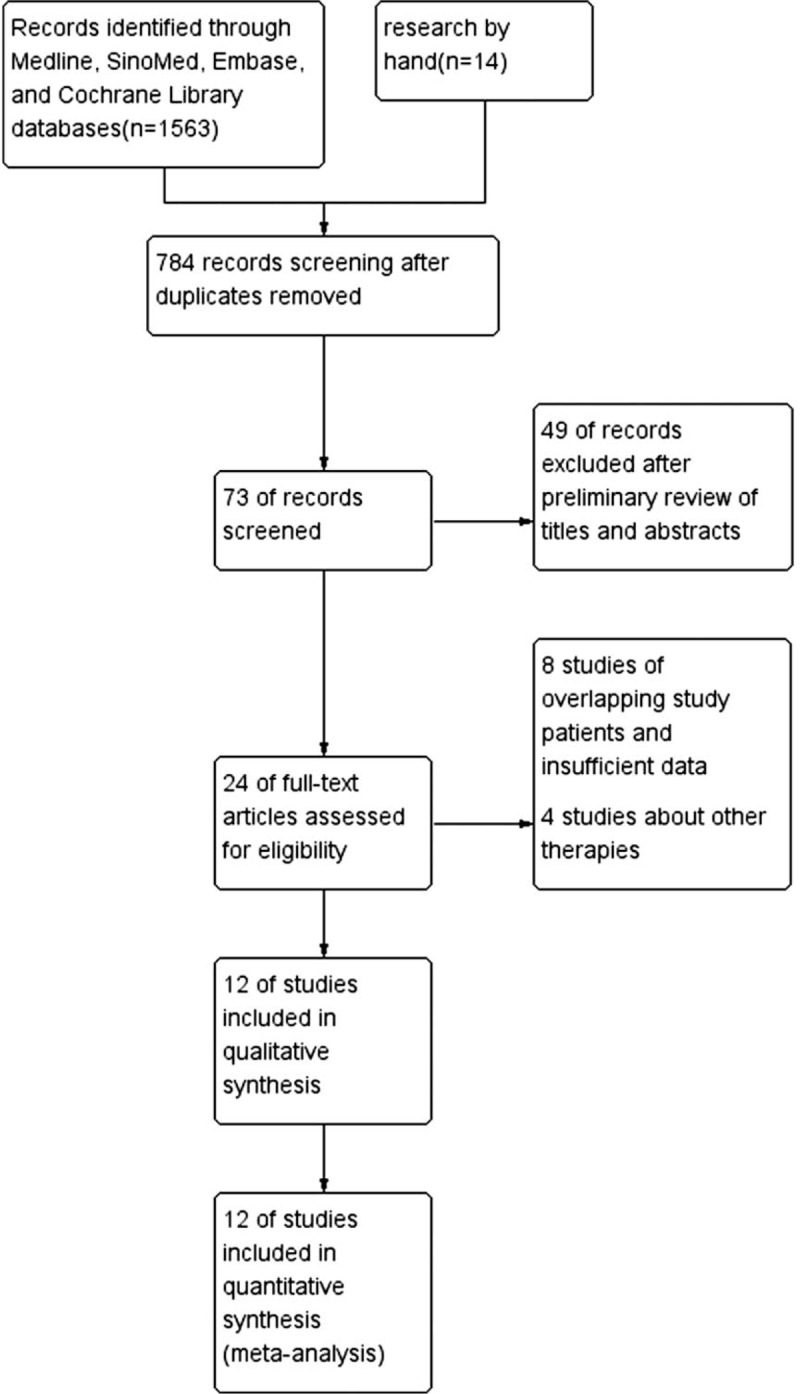
Methods: Four databases (Medline, SinoMed, EMBASE, and Cochrane Library) were searched for eligible studies from 1980 to 2018 containing a total of 4 randomized controlled trials and 8 prospective studies.
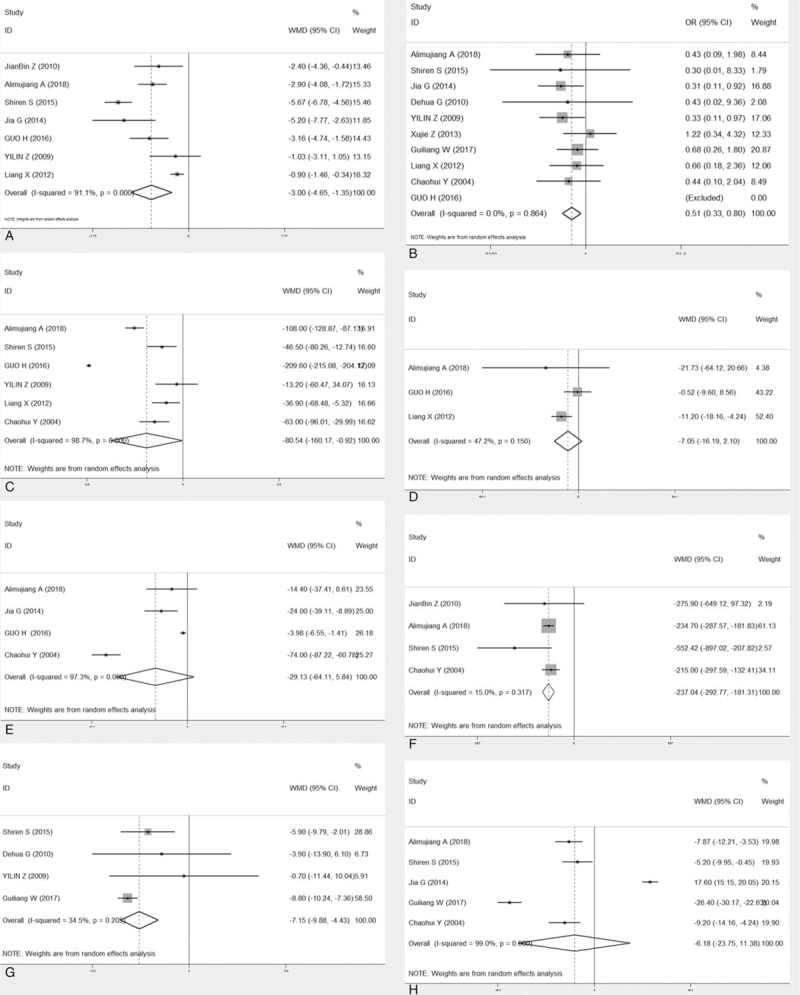
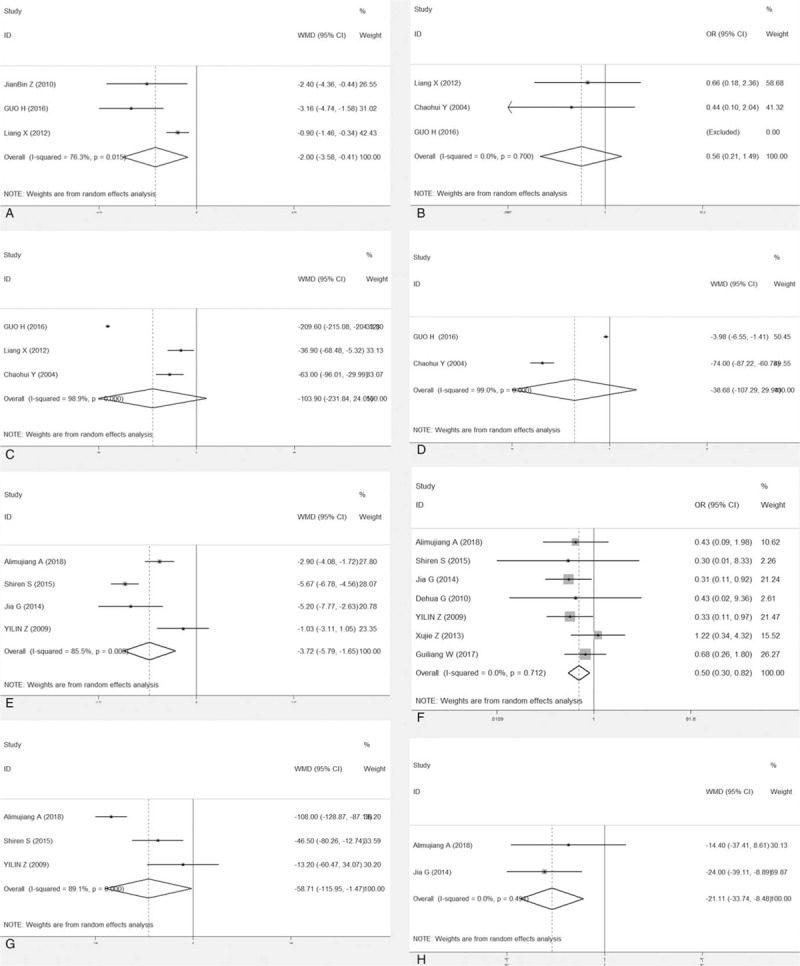
Results: After the analysis of data amenable to polling, significant advantages were found in favor of the CBP approach in terms of Acute Physiology and Chronic Health Evaluation II (APACHE II) score (WMD = -3.00,95%CI = -4.65 to -1.35), serum amylase (WMD = -237.14, 95% CI = -292.77 to 181.31), serum creatinine (WMD = -80.54,95%CI = 160.17 to -0.92), length of stay in the ICU (WMD = -7.15,95%CI = -9.88 to -4.43), and mortality (OR = 0.60, 95%CI = 0.38-0.94). No marked differences were found in terms of C-reactive protein (CRP), alamine aminotransferase (ALT) and length of hospital stay (LOS).
Conclusion: Compared with conventional treatment, CBP remedy evidently improved clinical outcomes, including reduced incidence organ failure, decreased serum amylase, APACHE II score, length of stay in the ICU and lower mortality rate, leading us to conclude that it is a safer treatment option for SAP. Furthermore, relevant multicenter RCTs are required to prove these findings.
Conflict of interest statement
There is no conflict of interest.
Figures
Similar articles
-
[Study on the clinical effect of initiating continuous blood purification at different times for severe acute pancreatitis].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024 Sep;36(9):937-942. doi: 10.3760/cma.j.cn121430-20240408-00317. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024. PMID: 39380514 Chinese.
-
Early gut barrier dysfunction in patients with severe acute pancreatitis: attenuated by continuous blood purification treatment.Int J Artif Organs. 2010 Oct;33(10):706-15. Int J Artif Organs. 2010. PMID: 21077043 Clinical Trial.
-
An endoscopic or minimally invasive surgical approach for infected necrotizing pancreatitis: a systematic review and meta-analysis.Rev Esp Enferm Dig. 2019 Jun;111(6):471-480. doi: 10.17235/reed.2019.5792/2018. Rev Esp Enferm Dig. 2019. PMID: 31021167
-
Continuous blood purification ameliorates endothelial hyperpermeability in SAP patients with MODS by regulating tight junction proteins via ROCK.Int J Artif Organs. 2013 Oct;36(10):700-9. doi: 10.5301/ijao.5000216. Epub 2013 Aug 2. Int J Artif Organs. 2013. PMID: 23918271
-
High-volume hemofiltration reduces short-term mortality with no influence on the incidence of MODS, hospital stay, and hospitalization cost in patients with severe-acute pancreatitis: A meta-analysis.Artif Organs. 2021 Dec;45(12):1456-1465. doi: 10.1111/aor.14016. Epub 2021 Jul 9. Artif Organs. 2021. PMID: 34240469
Cited by
-
Early continuous blood purification affects TNF-α, IL-1β, and IL-6 in patients with severe acute pancreatitis via inhibiting TLR4 signaling pathway.Kaohsiung J Med Sci. 2022 May;38(5):479-485. doi: 10.1002/kjm2.12497. Epub 2022 Jan 20. Kaohsiung J Med Sci. 2022. PMID: 35049137 Free PMC article. Clinical Trial.
-
Admission hematocrit and fluctuating blood urea nitrogen levels predict the efficacy of blood purification treatment in severe acute pancreatitis patients.J Artif Organs. 2025 Sep;28(3):431-438. doi: 10.1007/s10047-025-01501-2. Epub 2025 Apr 25. J Artif Organs. 2025. PMID: 40278997
-
Continuous Hemofiltration Reduces Mortality in Severe Acute Pancreatitis: A Meta-Analysis.Emerg Med Int. 2020 Jun 29;2020:6474308. doi: 10.1155/2020/6474308. eCollection 2020. Emerg Med Int. 2020. PMID: 32670639 Free PMC article.
-
CT Image Features Based on the Reconstruction Algorithm for Continuous Blood Purification Combined with Nursing Intervention in the Treatment of Severe Acute Pancreatitis.Contrast Media Mol Imaging. 2022 Mar 28;2022:2622316. doi: 10.1155/2022/2622316. eCollection 2022. Contrast Media Mol Imaging. 2022. PMID: 35414803 Free PMC article.
-
Clinical efficacy of blood purification using a polymethylmethacrylate hemofilter for the treatment of severe acute pancreatitis.Acute Crit Care. 2022 Aug;37(3):398-406. doi: 10.4266/acc.2022.00192. Epub 2022 Jul 5. Acute Crit Care. 2022. PMID: 35791651 Free PMC article.
References
-
- Lankisch PG, Apte M, Banks PA. Acute pancreatitis. Lancet 2015;386:85–96. - PubMed
-
- Johnson CD, Besselink MG, Carter R. Acute pancreatitis. BMJ (Clinical research ed) 2014;349:g4859. - PubMed
-
- van Dijk SM, Hallensleben NDL, van Santvoort HC, et al. Acute pancreatitis: recent advances through randomised trials. Gut 2017;66:2024–32. - PubMed
-
- Vege SS, DiMagno MJ, Forsmark CE, et al. Initial medical treatment of acute pancreatitis: American gastroenterological association institute technical review. Gastroenterology 2018;154:1103–39. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
