

Driver Mutations in Normal Airway Epithelium Elucidate Spatiotemporal Resolution of Lung Cancer
- PMID: 30896962
- PMCID: PMC6775870
- DOI: 10.1164/rccm.201806-1178OC
Driver Mutations in Normal Airway Epithelium Elucidate Spatiotemporal Resolution of Lung Cancer
Abstract
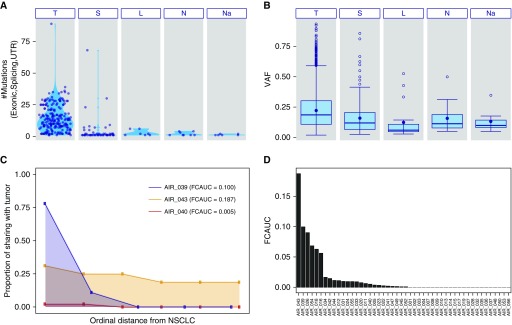
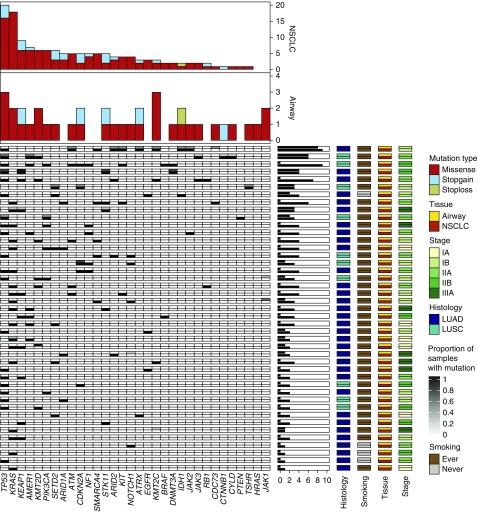
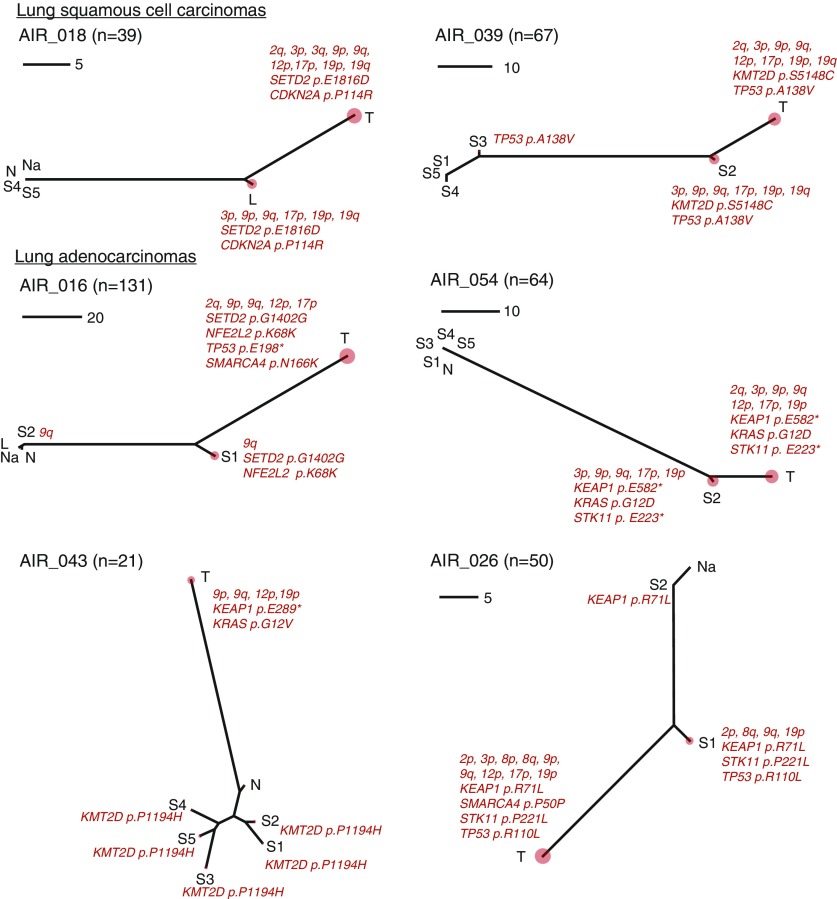
Rationale: Uninvolved normal-appearing airway epithelium has been shown to exhibit specific mutations characteristic of nearby non-small cell lung cancers (NSCLCs). Yet, its somatic mutational landscape in patients with early-stage NSCLC is unknown.Objectives: To comprehensively survey the somatic mutational architecture of the normal airway epithelium in patients with early-stage NSCLC.Methods: Multiregion normal airways, comprising tumor-adjacent small airways, tumor-distant large airways, nasal epithelium and uninvolved normal lung (collectively airway field), matched NSCLCs, and blood cells (n = 498) from 48 patients were interrogated for somatic single-nucleotide variants by deep-targeted DNA sequencing and for chromosomal allelic imbalance events by genome-wide genotype array profiling. Spatiotemporal relationships between the airway field and NSCLCs were assessed by phylogenetic analysis.Measurements and Main Results: Genomic airway field carcinogenesis was observed in 25 cases (52%). The airway field epithelium exhibited a total of 269 somatic mutations in most patients (n = 36) including key drivers that were shared with the NSCLCs. Allele frequencies of these acquired variants were overall higher in NSCLCs. Integrative analysis of single-nucleotide variants and allelic imbalance events revealed driver genes with shared "two-hit" alterations in the airway field (e.g., TP53, KRAS, KEAP1, STK11, and CDKN2A) and those with single hits progressing to two in the NSCLCs (e.g., PIK3CA and NOTCH1).Conclusions: Tumor-adjacent and tumor-distant normal-appearing airway epithelia exhibit somatic driver alterations that undergo selection-driven clonal expansion in NSCLC. These events offer spatiotemporal insights into the development of NSCLC and, thus, potential targets for early treatment.
Keywords: allelic imbalance; cancerization field; deep targeted sequencing; early-stage non–small cell lung cancer; normal airway.
Figures

Comment in
-
Sequencing Lung Cancer's Sequence.Am J Respir Crit Care Med. 2019 Sep 15;200(6):657-659. doi: 10.1164/rccm.201904-0837ED. Am J Respir Crit Care Med. 2019. PMID: 31059279 Free PMC article. No abstract available.
References
-
- Slaughter DP, Southwick HW, Smejkal W. Field cancerization in oral stratified squamous epithelium; clinical implications of multicentric origin. Cancer. 1953;6:963–968. - PubMed
-
- Curtius K, Wright NA, Graham TA. An evolutionary perspective on field cancerization. Nat Rev Cancer. 2018;18:19–32. - PubMed
-
- Braakhuis BJ, Tabor MP, Kummer JA, Leemans CR, Brakenhoff RH. A genetic explanation of Slaughter’s concept of field cancerization: evidence and clinical implications. Cancer Res. 2003;63:1727–1730. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68:7–30. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
