

Independent and combined effects of improved water, sanitation, and hygiene (WASH) and improved complementary feeding on early neurodevelopment among children born to HIV-negative mothers in rural Zimbabwe: Substudy of a cluster-randomized trial
- PMID: 30897095
- PMCID: PMC6428259
- DOI: 10.1371/journal.pmed.1002766
Independent and combined effects of improved water, sanitation, and hygiene (WASH) and improved complementary feeding on early neurodevelopment among children born to HIV-negative mothers in rural Zimbabwe: Substudy of a cluster-randomized trial
Abstract
Background: Globally, nearly 250 million children (43% of all children under 5 years of age) are at risk of compromised neurodevelopment due to poverty, stunting, and lack of stimulation. We tested the independent and combined effects of improved water, sanitation, and hygiene (WASH) and improved infant and young child feeding (IYCF) on early child development (ECD) among children enrolled in the Sanitation Hygiene Infant Nutrition Efficacy (SHINE) trial in rural Zimbabwe.
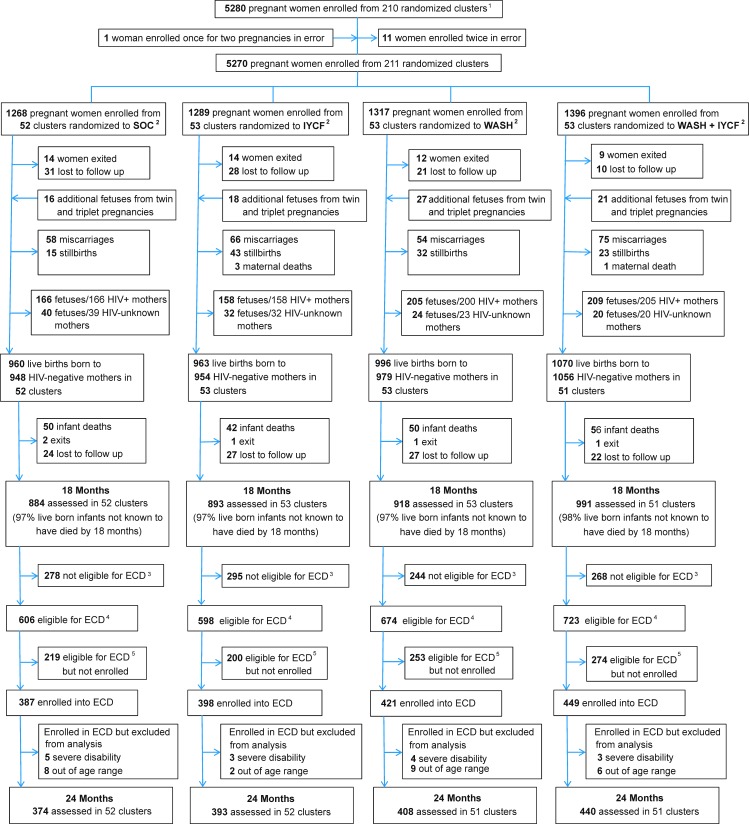
Methods and findings: SHINE was a cluster-randomized community-based 2×2 factorial trial. A total of 5,280 pregnant women were enrolled from 211 clusters (defined as the catchment area of 1-4 village health workers [VHWs] employed by the Zimbabwean Ministry of Health and Child Care). Clusters were randomly allocated to standard of care, IYCF (20 g of small-quantity lipid-based nutrient supplement per day from age 6 to 18 months plus complementary feeding counseling), WASH (ventilated improved pit latrine, handwashing stations, chlorine, liquid soap, and play yard), and WASH + IYCF. Primary outcomes were child length-for-age Z-score and hemoglobin concentration at 18 months of age. Children who completed the 18-month visit and turned 2 years (102-112 weeks) between March 1, 2016, and April 30, 2017, were eligible for the ECD substudy. We prespecified that primary inferences would be drawn from findings of children born to HIV-negative mothers; these results are presented in this paper. A total of 1,655 HIV-unexposed children (64% of those eligible) were recruited into the ECD substudy from 206 clusters and evaluated for ECD at 2 years of age using the Malawi Developmental Assessment Tool (MDAT) to assess gross motor, fine motor, language, and social skills; the MacArthur-Bates Communicative Development Inventories (CDI) to assess vocabulary and grammar; the A-not-B test to assess object permanence; and a self-control task. Outcomes were analyzed in the intention-to-treat population. For all ECD outcomes, there was not a statistical interaction between the IYCF and WASH interventions, so we estimated the effects of the interventions by comparing the 2 IYCF groups with the 2 non-IYCF groups and the 2 WASH groups with the 2 non-WASH groups. The mean (95% CI) total MDAT score was modestly higher in the IYCF groups compared to the non-IYCF groups in unadjusted analysis: 1.35 (0.24, 2.46; p = 0.017); this difference did not persist in adjusted analysis: 0.79 (-0.22, 1.68; p = 0.057). There was no evidence of impact of the IYCF intervention on the CDI, A-not-B, or self-control tests. Among children in the WASH groups compared to those in the non-WASH groups, mean scores were not different for the MDAT, A-not-B, or self-control tests; mean CDI score was not different in unadjusted analysis (0.99 [95% CI -1.18, 3.17]) but was higher in children in the WASH groups in adjusted analysis (1.81 [0.01, 3.61]). The main limitation of the study was the specific time window for substudy recruitment, meaning not all children from the main trial were enrolled.
Conclusions: We found little evidence that the IYCF and WASH interventions implemented in SHINE caused clinically important improvements in child development at 2 years of age. Interventions that directly target neurodevelopment (e.g., early stimulation) or that more comprehensively address the multifactorial nature of neurodevelopment may be required to support healthy development of vulnerable children.
Trial registration: ClinicalTrials.gov NCT01824940.
Conflict of interest statement
The authors have declared no competing interests exist.
Figures
Similar articles
-
Effects of improved complementary feeding and improved water, sanitation and hygiene on early child development among HIV-exposed children: substudy of a cluster randomised trial in rural Zimbabwe.BMJ Glob Health. 2020 Jan 13;5(1):e001718. doi: 10.1136/bmjgh-2019-001718. eCollection 2020. BMJ Glob Health. 2020. PMID: 32133164 Free PMC article. Clinical Trial.
-
Independent and combined effects of improved water, sanitation, and hygiene, and improved complementary feeding, on child stunting and anaemia in rural Zimbabwe: a cluster-randomised trial.Lancet Glob Health. 2019 Jan;7(1):e132-e147. doi: 10.1016/S2214-109X(18)30374-7. Lancet Glob Health. 2019. PMID: 30554749 Free PMC article. Clinical Trial.
-
Independent and combined effects of improved water, sanitation, and hygiene, and improved complementary feeding, on stunting and anaemia among HIV-exposed children in rural Zimbabwe: a cluster-randomised controlled trial.Lancet Child Adolesc Health. 2019 Feb;3(2):77-90. doi: 10.1016/S2352-4642(18)30340-7. Epub 2018 Dec 18. Lancet Child Adolesc Health. 2019. PMID: 30573417 Free PMC article. Clinical Trial.
-
Summarizing the Child Growth and Diarrhea Findings of the Water, Sanitation, and Hygiene Benefits and Sanitation Hygiene Infant Nutrition Efficacy Trials.Nestle Nutr Inst Workshop Ser. 2020;93:153-166. doi: 10.1159/000503350. Epub 2020 Jan 28. Nestle Nutr Inst Workshop Ser. 2020. PMID: 31991427 Review.
-
Effects of single and combined water, sanitation and hygiene (WASH) interventions on nutritional status of children: a systematic review and meta-analysis.Ital J Pediatr. 2019 Jul 4;45(1):77. doi: 10.1186/s13052-019-0666-2. Ital J Pediatr. 2019. PMID: 31272479 Free PMC article.
Cited by
-
Antenatal and delivery practices and neonatal mortality amongst women with institutional and non-institutional deliveries in rural Zimbabwe: observational data from a cluster randomized trial.BMC Pregnancy Childbirth. 2022 Dec 30;22(1):981. doi: 10.1186/s12884-022-05282-x. BMC Pregnancy Childbirth. 2022. PMID: 36585673 Free PMC article. Clinical Trial.
-
Cognitive Outcomes at 18 Months: Findings from the Early Life Interventions for Childhood Growth and Development in Tanzania (ELICIT) Trial.Am J Trop Med Hyg. 2021 Dec 6;106(2):441-445. doi: 10.4269/ajtmh.21-0596. Am J Trop Med Hyg. 2021. PMID: 34872064 Free PMC article. Clinical Trial.
-
School-age growth and development following infant feeding and/or water, sanitation, and hygiene interventions in rural Zimbabwe: long-term follow-up of a cluster-randomised trial.EClinicalMedicine. 2024 Nov 22;78:102946. doi: 10.1016/j.eclinm.2024.102946. eCollection 2024 Dec. EClinicalMedicine. 2024. PMID: 39640932 Free PMC article.
-
Under-nutrition and associated factors among children on ART in Southern Ethiopia: a facility-based cross-sectional study.Ital J Pediatr. 2021 Oct 11;47(1):205. doi: 10.1186/s13052-021-01154-w. Ital J Pediatr. 2021. PMID: 34635139 Free PMC article.
-
Effects of improved complementary feeding and improved water, sanitation and hygiene on early child development among HIV-exposed children: substudy of a cluster randomised trial in rural Zimbabwe.BMJ Glob Health. 2020 Jan 13;5(1):e001718. doi: 10.1136/bmjgh-2019-001718. eCollection 2020. BMJ Glob Health. 2020. PMID: 32133164 Free PMC article. Clinical Trial.
References
-
- United Nations Children’s Fund. Malnutrition. New York: United Nations Children’s Fund; 2018 [cited 2018 Oct 11]. Available from: https://data.unicef.org/topic/nutrition/malnutrition/.
-
- World Health Organization, United Nations Children’s Fund, World Bank Group. Levels and trends in child malnutrition: UNICEF/WHO/World Bank Group joint child malnutrition estimates—key findings of the 2018 edition. Geneva: World Health Organization; 2018.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
