

Two-photon fluorescence and second harmonic generation characterization of extracellular matrix remodeling in post-injury murine temporomandibular joint osteoarthritis
- PMID: 30897138
- PMCID: PMC6428409
- DOI: 10.1371/journal.pone.0214072
Two-photon fluorescence and second harmonic generation characterization of extracellular matrix remodeling in post-injury murine temporomandibular joint osteoarthritis
Abstract
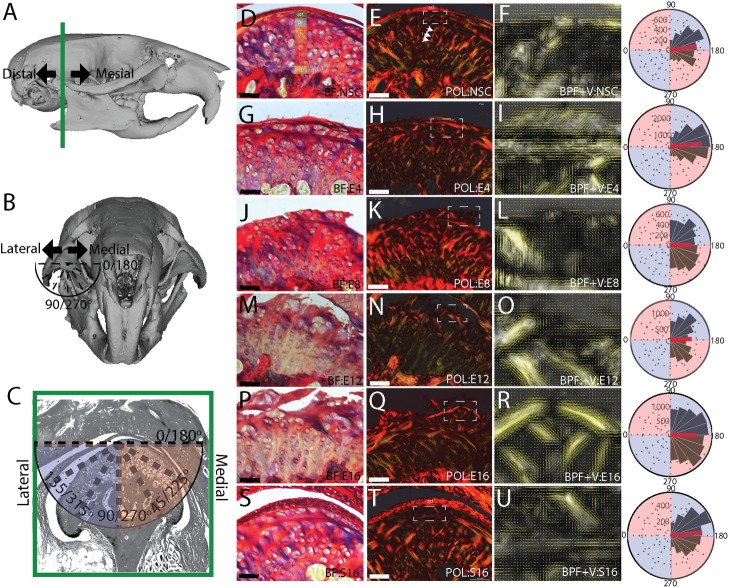
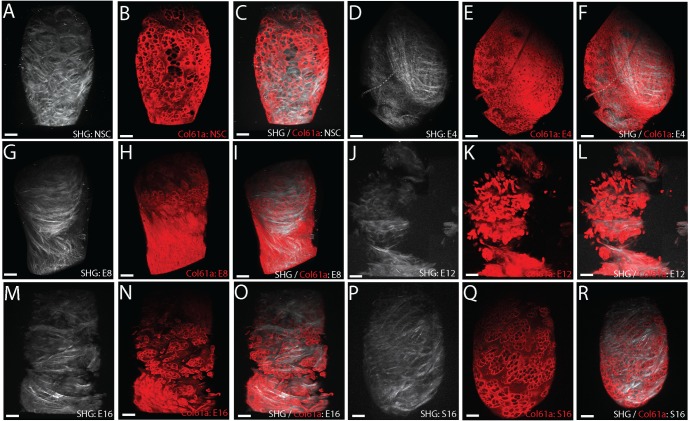
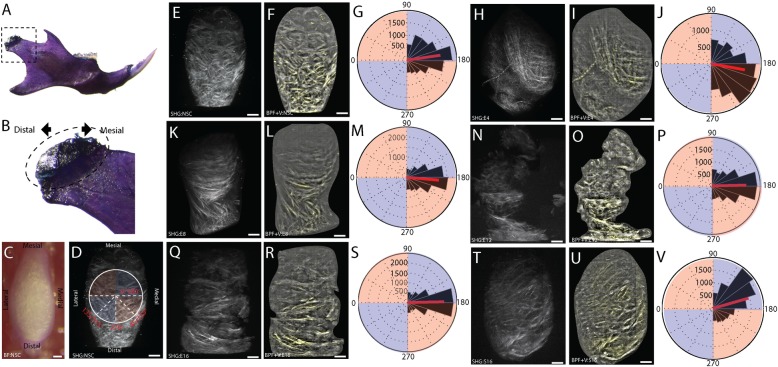
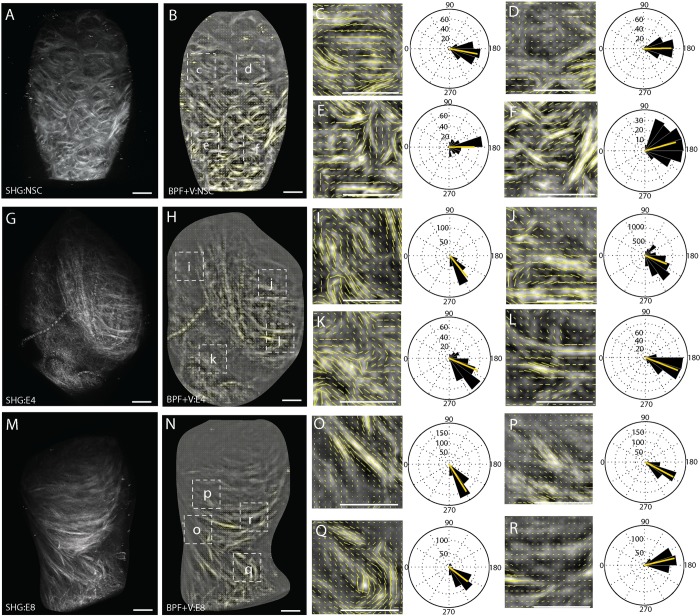
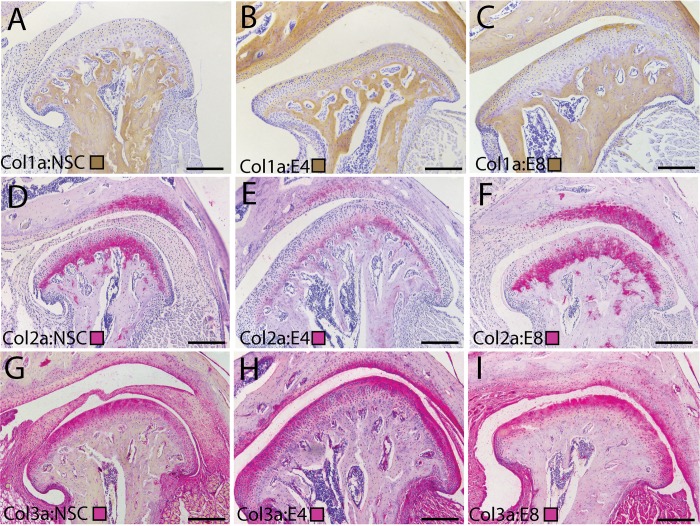
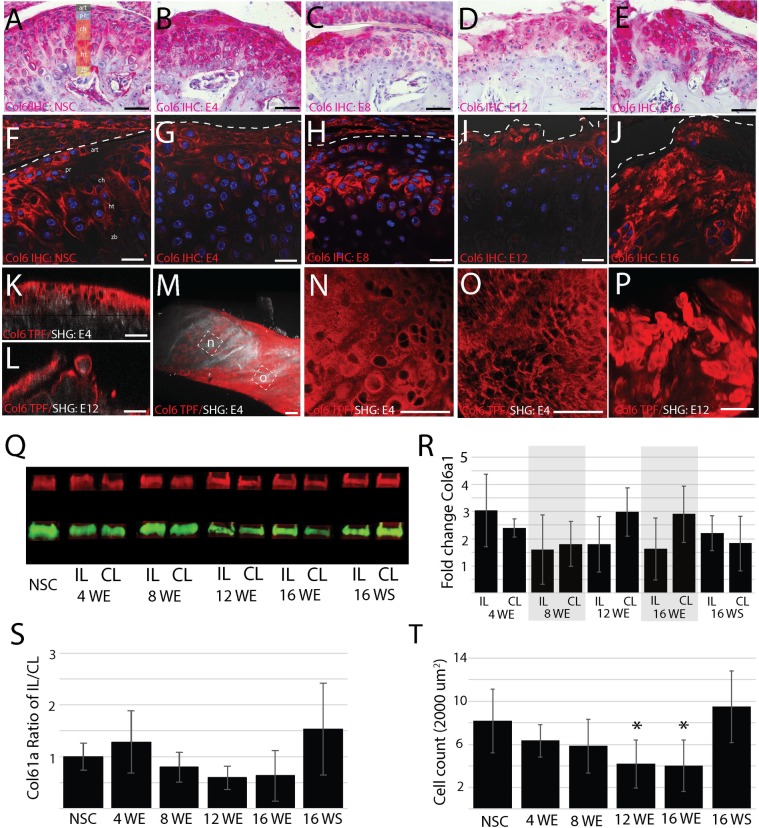
End stage temporomandibular joint osteoarthritis (TMJ-OA) is characterized by fibrillations, fissures, clefts, and erosion of the mandibular condylar cartilage. The goal of this study was to define changes in pericellular and interterritorial delineations of the extracellular matrix (ECM) that occur preceding and concurrent with the development of this end stage degeneration in a murine surgical instability model. Two-photon fluorescence (TPF) and second harmonic generation (SHG) microscopy was used to evaluate TMJ-OA mediated changes in the ECM. We illustrate that TPF/SHG microscopy reconstructs the three-dimensional network of key fibrillar and micro-fibrillar collagens altered during the progression of TMJ-OA. This method not only generates spatially distinct pericellular and interterritorial delineations of the ECM but distinguishes early and end stage TMJ-OA by signal organization, orientation, and composition. Early stage TMJ-OA at 4- and 8-weeks post-injury is characterized by two structurally distinct regions containing dense, large fiber collagens and superficial, small fiber collagens rich in types I, III, and VI collagen oriented along the mesiodistal axis of the condyle. At 8-weeks post-injury, type VI collagen is locally diminished on the central and medial condyle, but the type I/III rich superficial layer is still present. Twelve- and 16-weeks post-injury mandibular cartilage is characteristic of end-stage disease, with hypocellularity and fibrillations, fissures, and clefts in the articular layer that propagate along the mediolateral axis of the MCC. We hypothesize that the localized depletion of interterritorial and pericellular type VI collagen may signify an early marker for the transition from early to end stage TMJ-OA, influence the injury response of the tissue, and underlie patterns of degeneration that follow attritional modes of failure.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Helmy E, Bays R, Sharawy M. Osteoarthrosis of the temporomandibular joint following experimental disc perforation in Macaca fascicularis. J Oral Maxillofac Surg. 1988;46(11):979–90. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
