

Cushing syndrome: uncovering Carney complex due to novel PRKAR1A mutation
- PMID: 30897549
- PMCID: PMC6432981
- DOI: 10.1530/EDM-18-0150
Cushing syndrome: uncovering Carney complex due to novel PRKAR1A mutation
Abstract
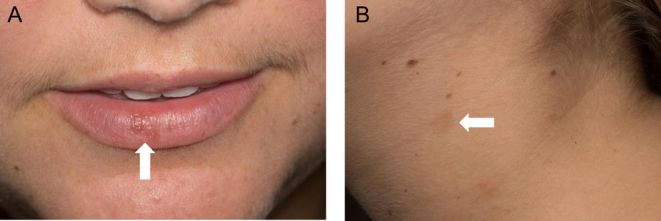
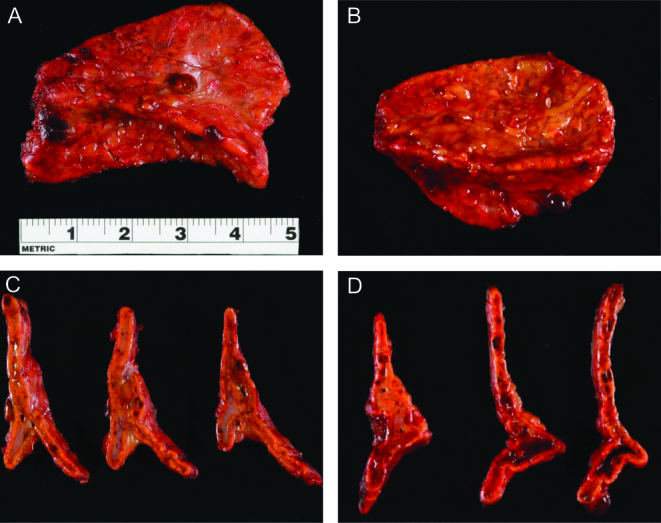
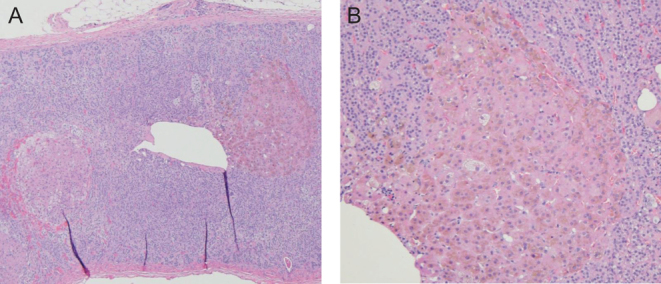
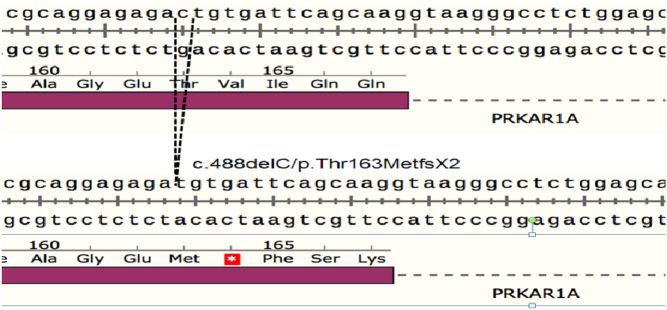
Carney complex (CNC) is a rare multiple neoplasia syndrome characterized by spotty pigmentation of the skin and mucosa in association with various non-endocrine and endocrine tumors, including primary pigmented nodular adrenocortical disease (PPNAD). A 20-year-old woman was referred for suspected Cushing syndrome. She had signs of cortisol excess as well as skin lentigines on physical examination. Biochemical investigation was suggestive of corticotropin (ACTH)-independent Cushing syndrome. Unenhanced computed tomography scan of the abdomen did not reveal an obvious adrenal mass. She subsequently underwent bilateral laparoscopic adrenalectomy, and histopathology was consistent with PPNAD. Genetic testing revealed a novel frameshift pathogenic variant c.488delC/p.Thr163MetfsX2 (ClinVar Variation ID: 424516) in the PRKAR1A gene, consistent with clinical suspicion for CNC. Evaluation for other clinical features of the complex was unrevealing. We present a case of PPNAD-associated Cushing syndrome leading to the diagnosis of CNC due to a novel PRKAR1A pathogenic variant. Learning points: PPNAD should be considered in the differential for ACTH-independent Cushing syndrome, especially when adrenal imaging appears normal. The diagnosis of PPNAD should prompt screening for CNC. CNC is a rare multiple neoplasia syndrome caused by inactivating pathogenic variants in the PRKAR1A gene. Timely diagnosis of CNC and careful surveillance can help prevent potentially fatal complications of the disease.
Keywords: 2019; ACTH; Adolescent/young adult; Adrenal; Adrenalectomy; Anxiety; Buffalo hump; CT scan; Carney complex; Cortisol; Cortisol (serum); Cushing's syndrome; DNA sequencing; Dehydroepiandrostenedione; Dexamethasone suppression (high dose); Dexamethasone suppression (low dose); Error in diagnosis/pitfalls and caveats; Facial plethora; Facies - moon; Female; Fludrocortisone; Genetics; Glucocorticoids; Haematoxylin and eosin staining; Hirsutism; Histopathology; Hydrocortisone; Laparoscopic adrenalectomy; March; Mineralocorticoids; Molecular genetic analysis; Necrosis; Obesity; Skin pigmentation - spotty; Striae; United States; Weight gain; White.
Figures

Similar articles
-
The clinical characteristics and pathogenic variants of primary pigmented nodular adrenocortical disease in 210 patients: a systematic review.Front Endocrinol (Lausanne). 2024 Jun 26;15:1356870. doi: 10.3389/fendo.2024.1356870. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 39006359 Free PMC article.
-
A case report and literature review of Carney complex with atrial adenomyxoma.BMC Endocr Disord. 2023 Feb 6;23(1):35. doi: 10.1186/s12902-023-01285-7. BMC Endocr Disord. 2023. PMID: 36740703 Free PMC article. Review.
-
PRKAR1A mutations in primary pigmented nodular adrenocortical disease.Pituitary. 2006;9(3):211-9. doi: 10.1007/s11102-006-0266-1. Pituitary. 2006. PMID: 17036196 Review.
-
Adrenal Cushing Syndrome: Diagnosis and Management in a 10-Year-Old Boy with Carney Complex.Horm Res Paediatr. 2024 Aug 5:1-10. doi: 10.1159/000540691. Online ahead of print. Horm Res Paediatr. 2024. PMID: 39102796
-
Mutations of the PRKAR1A gene in Cushing's syndrome due to sporadic primary pigmented nodular adrenocortical disease.J Clin Endocrinol Metab. 2002 Sep;87(9):4324-9. doi: 10.1210/jc.2002-020592. J Clin Endocrinol Metab. 2002. PMID: 12213893
Cited by
-
Treatment of Primary Pigmented Nodular Adrenocortical Disease.Horm Metab Res. 2022 Nov;54(11):721-730. doi: 10.1055/a-1948-6990. Epub 2022 Sep 21. Horm Metab Res. 2022. PMID: 36130700 Free PMC article. Review.
-
The clinical characteristics and pathogenic variants of primary pigmented nodular adrenocortical disease in 210 patients: a systematic review.Front Endocrinol (Lausanne). 2024 Jun 26;15:1356870. doi: 10.3389/fendo.2024.1356870. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 39006359 Free PMC article.
-
A Novel Missense PRKAR1A Variant Causes Carney Complex.Endocrinol Metab (Seoul). 2022 Oct;37(5):810-815. doi: 10.3803/EnM.2022.1544. Epub 2022 Oct 4. Endocrinol Metab (Seoul). 2022. PMID: 36193716 Free PMC article.
References
-
- Bertherat J, Horvath A, Groussin L, Grabar S, Boikos S, Cazabat L, Libe R, Rene-Corail F, Stergiopoulos S, Bourdeau I, et al Mutations in regulatory subunit type 1A of cyclic adenosine 5′-monophosphate-dependent protein kinase (PRKAR1a): phenotype analysis on 353 patients and 80 different genotypes. Journal of Clinical Endocrinology and Metabolism 2009. 94 2085–2091. (10.1210/jc.2008-2333) - DOI - PMC - PubMed
-
- Courcoutsakis NA, Tatsi C, Patronas NJ, Lee CC, Prassopoulos PK, Stratakis CA. The complex of myxomas, spotty skin pigmentation and endocrine overactivity (Carney complex): imaging findings with clinical and pathological correlation. Insights into Imaging 2013. 4 119–133. (10.1007/s13244-012-0208-6) - DOI - PMC - PubMed
-
- Stratakis CA, Sarlis N, Kirschner LS, Carney JA, Doppman JL, Nieman LK, Chrousos GP, Papanicolaou DA. Paradoxical response to dexamethasone in the diagnosis of primary pigmented nodular adrenocortical disease. Annals of Internal Medicine 1999. 131 585–591. (10.7326/0003-4819-131-8-199910190-00006) - DOI - PubMed
LinkOut - more resources
Full Text Sources
