

Prognostic Value of Left Ventricular Function and Mechanics in Pulmonary Hypertension: A Pilot Cardiovascular Magnetic Resonance Feature Tracking Study
- PMID: 30897834
- PMCID: PMC6473343
- DOI: 10.3390/medicina55030073
Prognostic Value of Left Ventricular Function and Mechanics in Pulmonary Hypertension: A Pilot Cardiovascular Magnetic Resonance Feature Tracking Study
Abstract
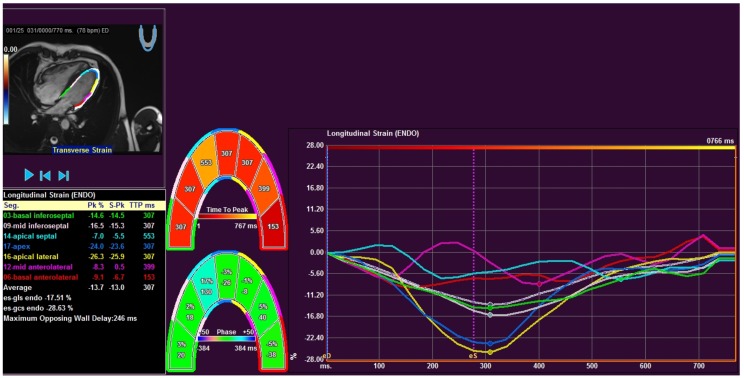
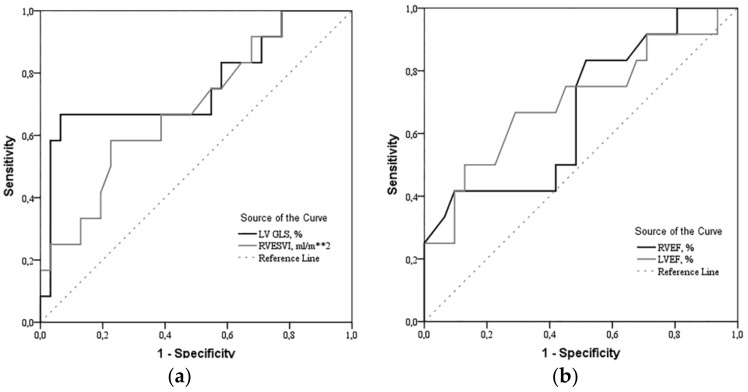
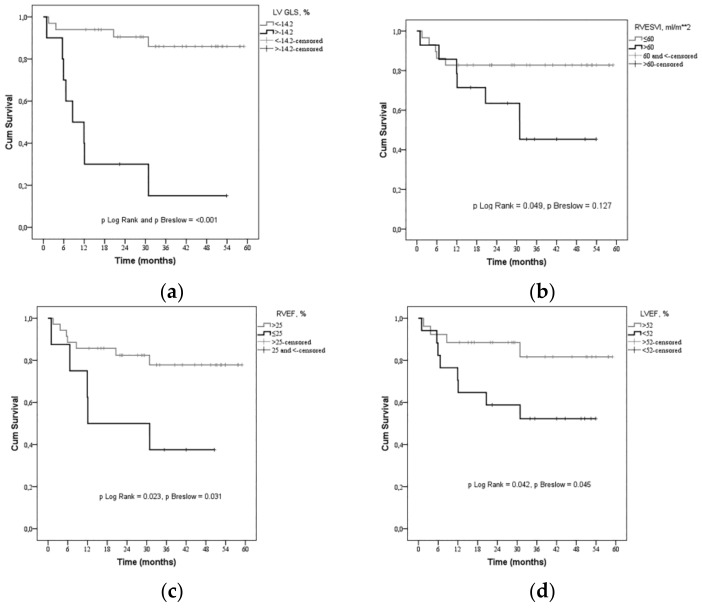
Background and objective: Cardiovascular magnetic resonance (CMR) - based feature tracking (FT) can detect left ventricular (LV) strain abnormalities in pulmonary hypertension (PH) patients, but little is known about the prognostic value of LV function and mechanics in PH patients. The aim of this study was to evaluate LV systolic function by conventional CMR and LV global strains by CMR-based FT analysis in precapillary PH patients, thereby defining the prognostic value of LV function and mechanics. Methods: We prospectively enrolled 43 patients with precapillary PH (mean pulmonary artery pressure (mPAP) 55.91 ± 15.87 mmHg, pulmonary arterial wedge pressure (PAWP) ≤15 mmHg) referred to CMR for PH evaluation. Using FT software, the LV global longitudinal strain (GLS) and global circumferential strain (GCS), also right ventricular (RV) GLS were analyzed. Results: Patients were classified into two groups according to survival (survival/non-survival). LV GLS was significantly reduced in the non-survival group (-12.4% [-19.0⁻(-7.8)] vs. -18.4% [-22.5⁻(-15.5)], p = 0.009). By ROC curve analysis, LV GLS > -14.2% (CI: 3.229 to 37.301, p < 0.001) was found to be robust predictor of mortality in PH patients. Univariable analysis using the Cox model showed that severely reduced LV GLS > -14.2%, with good sensitivity (77.8%) and high specificity (93.5%) indicated an increase of the risk of death by 11-fold. LV GLS significantly correlated in PH patients with RV ESVI (r = 0.322, p = 0.035), RV EF (r = 0.444, p < 0.003). Conclusions: LV systolic function and LV global longitudinal strain measurements using CMR-FT correlates with RV dysfunction and is associated with poor clinical outcomes in precapillary PH patients.
Keywords: cardiovascular magnetic resonance.; feature tracking; left ventricular; pulmonary hypertension.
Conflict of interest statement
The authors report no relationships that could be construed as a conflict of interest.
Figures
References
-
- Swift A.J., Rajaram S., Campbell M.J., Hurdman J., Thomas S., Capener D., Elliot C., Condliffe R., Wild J.M., Kiely D.G. Prognostic value of cardiovascular magnetic resonance imaging measurements corrected for age and sex in idiopathic pulmonary arterial hypertension. Circ. Cardiovasc. Imaging. 2014;7:100–106. doi: 10.1161/CIRCIMAGING.113.000338. - DOI - PubMed
-
- Van De Veerdonk M.C., Kind T., Marcus J.T., Mauritz G.-J., Heymans M.W., Bogaard H.-J., Boonstra A., Marques K.M., Westerhof N., Vonk-Noordegraaf A. Progressive right ventricular dysfunction in patients with pulmonary arterial hypertension responding to therapy. J. Am. Coll. Cardiol. 2011;58:2511–2519. doi: 10.1016/j.jacc.2011.06.068. - DOI - PubMed
-
- Swift A.J., Capener D., Johns C., Hamilton N., Rothman A., Elliot C., Condliffe R., Charalampopoulos A., Rajaram S., Lawrie A., et al. Magnetic resonance imaging in the prognostic evaluation of patients with pulmonary arterial hypertension. Am. J. Respir. Crit. Care Med. 2017;196:228–239. doi: 10.1164/rccm.201611-2365OC. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
