

Association of Lowering Low-Density Lipoprotein Cholesterol With Contemporary Lipid-Lowering Therapies and Risk of Diabetes Mellitus: A Systematic Review and Meta-Analysis
- PMID: 30898075
- PMCID: PMC6509736
- DOI: 10.1161/JAHA.118.011581
Association of Lowering Low-Density Lipoprotein Cholesterol With Contemporary Lipid-Lowering Therapies and Risk of Diabetes Mellitus: A Systematic Review and Meta-Analysis
Abstract
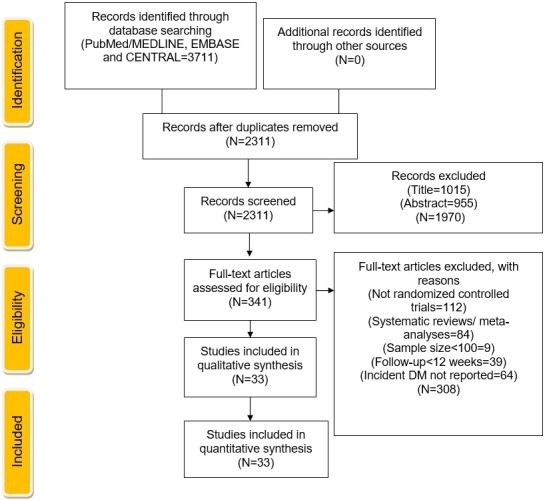
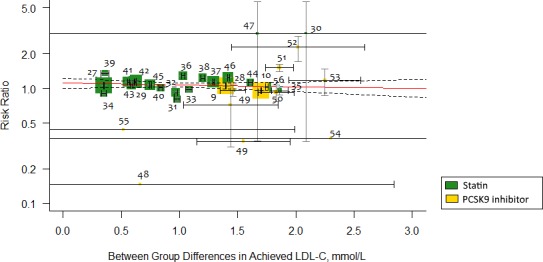
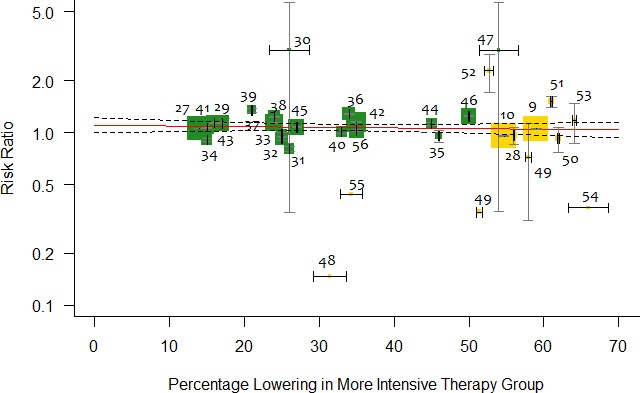
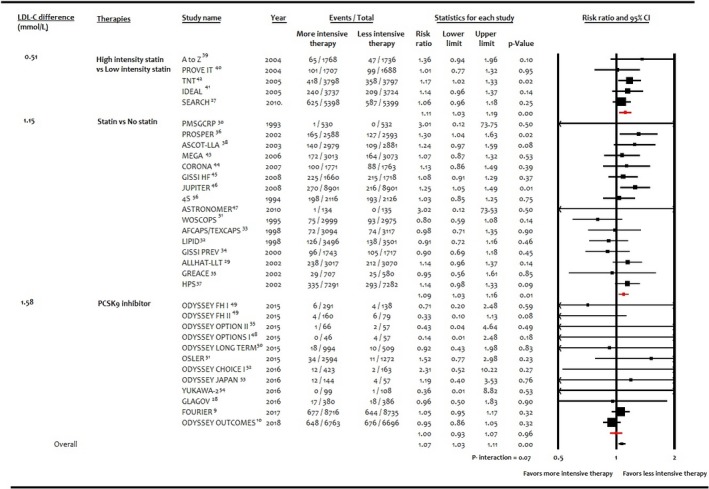
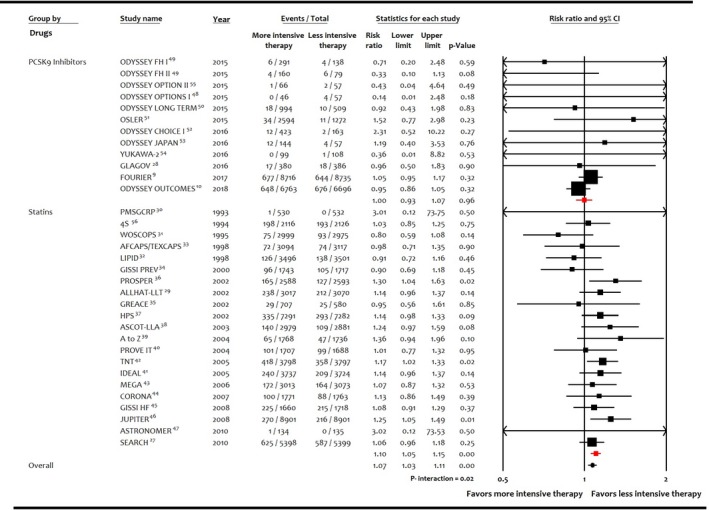
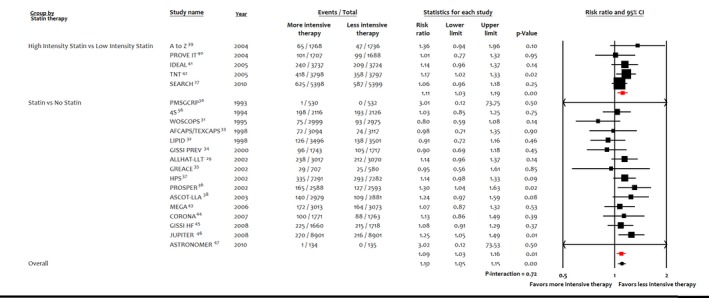
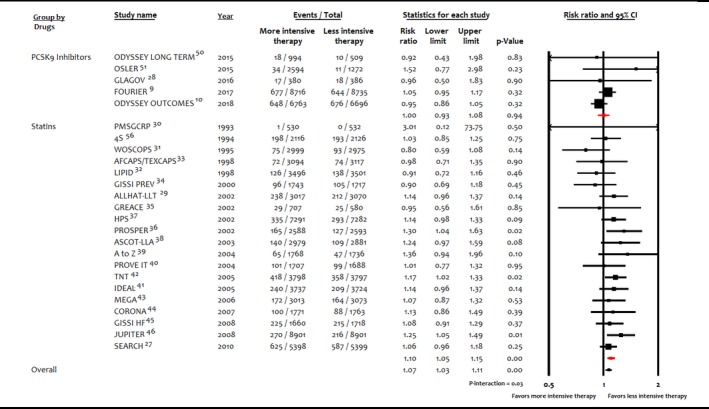
Background The relationship between lowering LDL (low-density lipoprotein) cholesterol with contemporary lipid-lowering therapies and incident diabetes mellitus ( DM ) remains uncertain. Methods and Results Thirty-three randomized controlled trials (21 of statins, 12 of PCSK9 [proprotein convertase subtilisin/kexin type 9] inhibitors, and 0 of ezetimibe) were selected using Medline , Embase, and the Cochrane Central Register of Controlled Trials (inception through November 15, 2018). A total of 163 688 nondiabetic patients were randomly assigned to more intensive (83 123 patients) or less intensive (80 565 patients) lipid-lowering therapy. More intensive lipid-lowering therapy was defined as the more potent pharmacological strategy ( PCSK 9 inhibitors, higher intensity statins, or statins), whereas less intensive therapy corresponded to active control group or placebo/usual care of the trial. Metaregression and meta-analyses were conducted using a random-effects model. No significant association was noted between 1-mmol/L reduction in LDL cholesterol and incident DM for more intensive lipid-lowering therapy (risk ratio: 0.95; 95% CI , 0.87-1.04; P=0.30; R2=14%) or for statins or PCSK 9 inhibitors. More intensive lipid-lowering therapy was associated with a higher risk of incident DM compared with less intensive therapy (risk ratio: 1.07; 95% CI , 1.03-1.11; P<0.001; I2=0%). These results were driven by higher risk of incident DM with statins (risk ratio: 1.10; 95% CI , 1.05-1.15; P<0.001; I2=0%), whereas PCSK 9 inhibitors were not associated with incident DM (risk ratio: 1.00; 95% CI , 0.93-1.07; P=0.96; I2=0%; P=0.02 for interaction). Conclusions Among intensive lipid-lowering therapies, there was no independent association between reduction in LDL cholesterol and incident DM . The risk of incident DM was higher with statins, whereas PCSK 9 inhibitors had no association with risk of incident DM .
Keywords: LDL (low‐density lipoprotein) cholesterol; PCSK9 (proprotein convertase subtilisin/kexin type 9); diabetes mellitus; statin.
Figures
References
-
- Silverman MG, Ference BA, Im K, Wiviott SD, Giugliano RP, Grundy SM, Braunwald E, Sabatine MS. Association between lowering LDL‐C and cardiovascular risk reduction among different therapeutic interventions: a systematic review and meta‐analysis. JAMA. 2016;316:1289–1297. - PubMed
-
- Koskinas KC, Siontis GCM, Piccolo R, Mavridis D, Raber L, Mach F, Windecker S. Effect of statins and non‐statin LDL‐lowering medications on cardiovascular outcomes in secondary prevention: a meta‐analysis of randomized trials. Eur Heart J. 2018;39:1172–1180. - PubMed
-
- Khan SU, Talluri S, Riaz H, Rahman H, Nasir F, Bin Riaz I, Sattur S, Ahmed H, Kaluski E, Krasuski R. A Bayesian network meta‐analysis of PCSK9 inhibitors, statins and ezetimibe with or without statins for cardiovascular outcomes. Eur J Prev Cardiol. 2018;25:844–853. DOI: 10.1177/2047487318766612. - DOI - PubMed
-
- Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, Goldberg AC, Gordon D, Levy D, Lloyd‐Jones DM, McBride P, Schwartz JS, Shero ST, Smith SC Jr, Watson K, Wilson PW. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63:2889–2934. - PubMed
-
- Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, Hoes AW, Jennings CS, Landmesser U, Pedersen TR, Reiner Z, Riccardi G, Taskinen MR, Tokgozoglu L, Verschuren WM, Vlachopoulos C, Wood DA, Zamorano JL. 2016 ESC/EAS guidelines for the management of dyslipidaemias. Eur Heart J. 2016;37:2999–3058. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
