

A population-based analysis of invasive fungal disease in haematology-oncology patients using data linkage of state-wide registries and administrative databases: 2005 - 2016
- PMID: 30898090
- PMCID: PMC6429824
- DOI: 10.1186/s12879-019-3901-y
A population-based analysis of invasive fungal disease in haematology-oncology patients using data linkage of state-wide registries and administrative databases: 2005 - 2016
Abstract
Background: Little is known about the morbidity and mortality of invasive fungal disease (IFD) at a population level. The aim of this study was to determine the incidence, trends and outcomes of IFD in all haematology-oncology patients by linking Victorian hospital data to state-based registries.
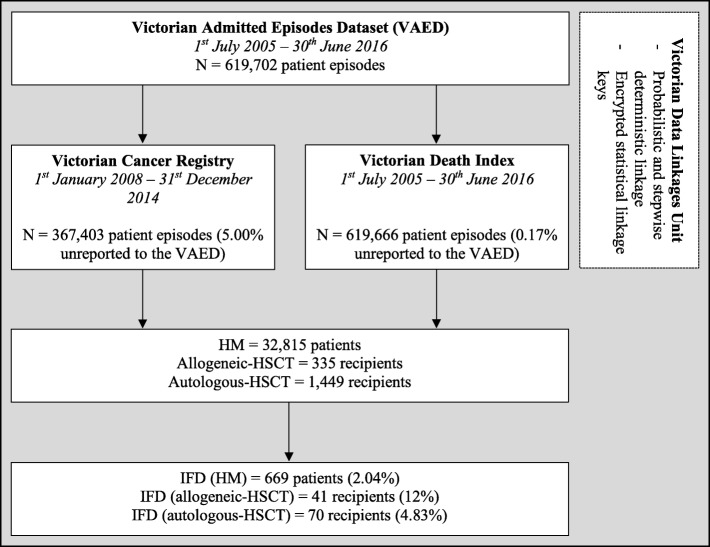
Methods: Episodes of IFD complicating adult haematological malignancy (HM) and haematopoietic stem cell transplantation (HSCT) patients admitted to Victorian hospitals from 1st July 2005 to 30th June 2016 were extracted from the Victorian Admitted Episodes Dataset and linked to the date of HM diagnosis from the Victorian Cancer Registry and mortality from the Victorian Death Index. Descriptive analyses and regression modelling were used.
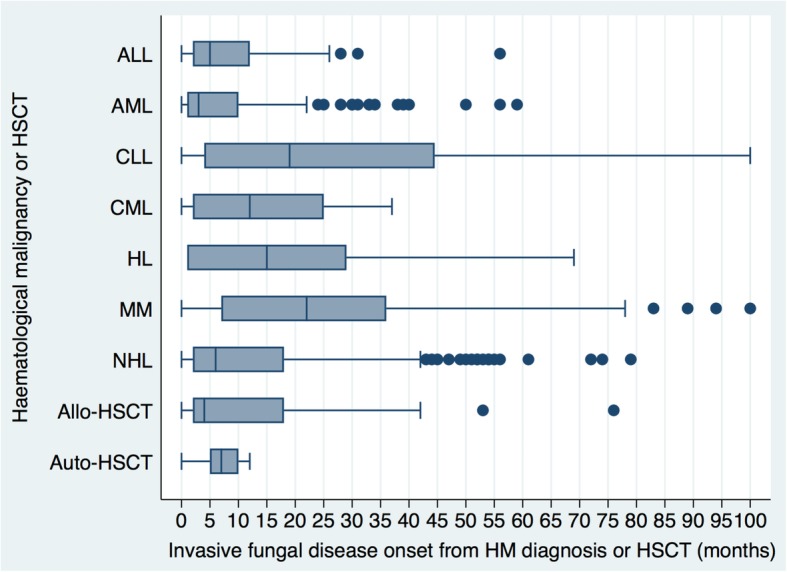
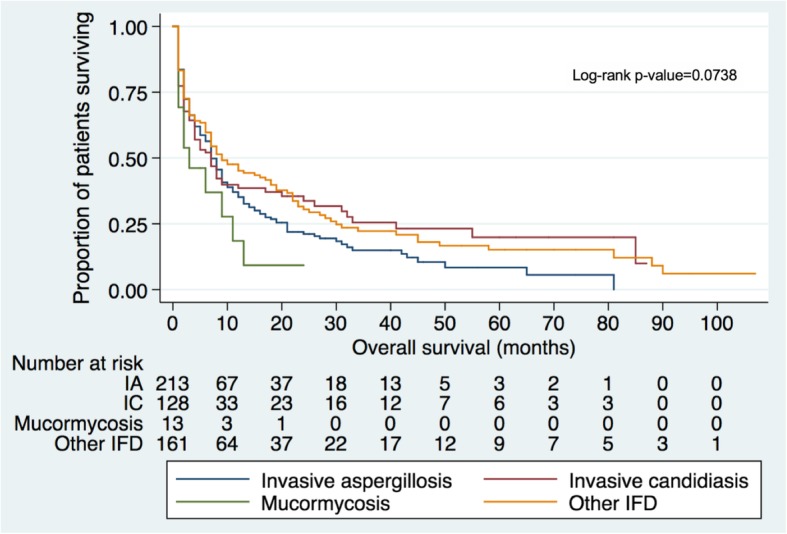
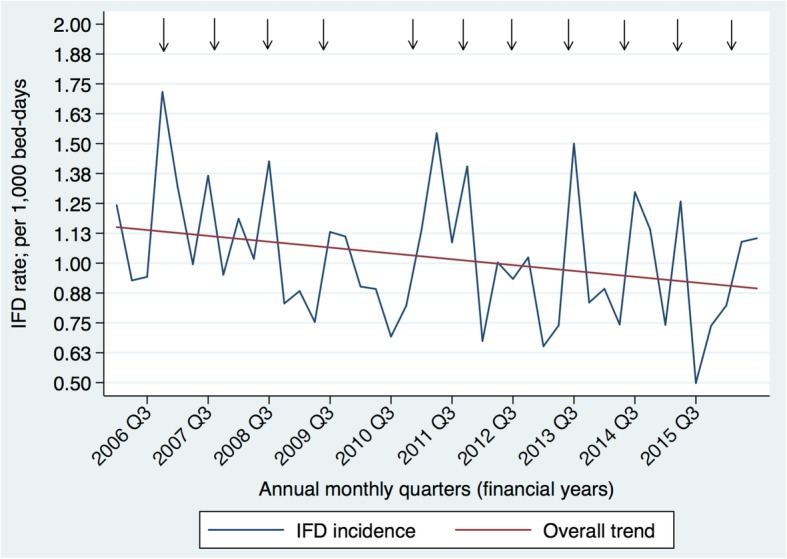
Results: There were 619,702 inpatient-episodes among 32,815 HM and 1,765 HSCT-patients. IFD occurring twelve-months from HM-diagnosis was detected in 669 (2.04%) HM-patients and 111 (6.29%) HSCT-recipients, respectively. Median time to IFD-diagnosis was 3, 5, 15 and 22 months in acute myeloid leukaemia, acute lymphoblastic leukaemia, Hodgkin lymphoma and multiple myeloma, respectively. Median survival from IFD-diagnosis was 7, 7 and 3 months for invasive aspergillosis, invasive candidiasis and mucormycosis, respectively. From 2005-2016, IFD incidence decreased 0.28% per 1,000 bed-days. Fungal incidence coincided with spring peaks on time-series analysis.
Conclusions: Data linkage is an efficient means of evaluating the epidemiology of a rare disease, however the burden of IFD is likely underestimated, arguing for better quality hospital level surveillance data to improve management strategies.
Keywords: Invasive fungal disease; data linkage; epidemiology; haematological malignancy; haematopoietic stem cell transplantation.
Conflict of interest statement
Authors’ information
J.C.V. BBiomedSc(Hons), Ph.D. Candidate and Research Fellow, University of Melbourne, the Peter MacCallum Cancer Centre and the National Centre for Infections in Cancer; C.O.M. MB, BCh, FRACP, Grad Dip Clin Epi, Ph.D., Infectious Diseases Physician, Monash University and Alfred Health; M.A.T. MBiostat, BSc., Research Fellow and Biostatistician, Austin Health; D.L.
Ethics approval and consent to participate
Written ethics approval was granted by the Alfred Health Human Research Ethics Committee (project number: 93/17). The need for informed consent was deemed unnecessary according to national regulations in accordance with the National Health and Medical Research Council
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Slavin M, van Hal S, Sorrell TC, Lee A, Marriott DJ, Daveson K, Kennedy K, Hajkowicz K, Halliday C, Athan E, et al. Invasive infections due to filamentous fungi other than Aspergillus: Epidemiology and determinants of mortality. Clin Microbiol Infect. 2015;21:490 e491–490 e410. doi: 10.1016/j.cmi.2014.12.021. - DOI - PubMed
-
- Even C, Bastuji-Garin S, Hicheri Y, Pautas C, Botterel F, Maury S, Cabanne L, Bretagne S, Cordonnier C. Impact of invasive fungal disease on the chemotherapy schedule and event-free survival in acute leukemia patients who survived fungal disease: A case-control study. Haematologica. 2011;96:337–341. doi: 10.3324/haematol.2010.030825. - DOI - PMC - PubMed
-
- Slavin M, Fastenau J, Sukarom I, Mavros P, Crowley S, Gerth WC. Burden of hospitalization of patients with Candida and Aspergillus infections in Australia. J Infect Dis Med. 2004;8:111–120. - PubMed
-
- Lingaratnam S, Thursky KA, Slavin MA, Kirsa SW, Bennett CA, Worth LJ. The disease and economic burden of neutropenic fever in adult patients in Australian cancer treatment centres 2008: Analysis of the Victorian Admitted Episodes Dataset. Intern Med J. 2011;41:121–129. doi: 10.1111/j.1445-5994.2010.02343.x. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
