

Second and third look laparoscopy in pT4 colon cancer patients for early detection of peritoneal metastases; the COLOPEC 2 randomized multicentre trial
- PMID: 30898098
- PMCID: PMC6429794
- DOI: 10.1186/s12885-019-5408-8
Second and third look laparoscopy in pT4 colon cancer patients for early detection of peritoneal metastases; the COLOPEC 2 randomized multicentre trial
Abstract
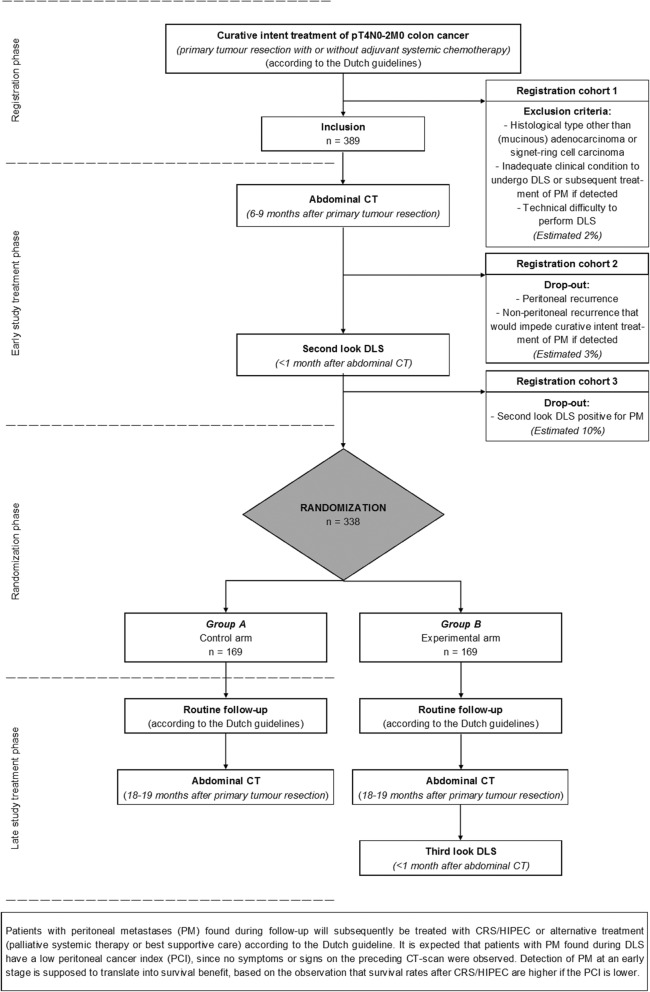
Background: Approximately 20-30% of patients with pT4 colon cancer develop metachronous peritoneal metastases (PM). Due to restricted accuracy of imaging modalities and absence of early symptoms, PM are often detected at a stage in which only a quarter of patients are eligible for curative intent treatment. Preliminary findings of the COLOPEC trial (NCT02231086) revealed that PM were already detected during surgical re-exploration within two months after primary resection in 9% of patients with pT4 colon cancer. Therefore, second look diagnostic laparoscopy (DLS) to detect PM at a subclinical stage may be considered an essential component of early follow-up in these patients, although this needs confirmation in a larger patient cohort. Furthermore, a third look DLS after a negative second look DLS might be beneficial for detection of PM occurring at a later stage.
Methods: The aim of this study is to determine the yield of second look DLS and added value of third look DLS after negative second look DLS in detecting occult PM in pT4N0-2 M0 colon cancer patients after completion of primary treatment. Patients will undergo an abdominal CT at 6 months postoperative, followed by a second look DLS within 1 month if no PM or other metastases not amenable for local treatment are detected. Patients without PM will subsequently be randomized between routine follow-up including 18 months abdominal CT, or an experimental arm with a third look DLS provided that PM or incurable metastases are absent at the 18 months abdominal CT. Primary endpoint is the proportion of PM detected after a negative second look DLS and will be determined at 20 months postoperative.
Discussion: Second look DLS is supposed to result in 10% occult PM, and third look DLS after negative second look DLS is expected to detect an additional 10% of PM compared to routine follow-up alone in patients with pT4 colon cancer. Detection of PM at an early stage will likely increase the proportion of patients eligible for curative intent treatment and subsequently improve survival, given the uniformly reported direct association between the extent of peritoneal disease and survival.
Trial registration: ClinicalTrials.gov: NCT03413254 , January 2018.
Keywords: Diagnostic laparoscopy; Early detection; Peritoneal metastases; Second/third look surgery; T4 colon cancer.
Conflict of interest statement
Ethics approval and consent to participate
The medical ethical committee of the Academic Medical Centre Amsterdam has approved the study protocol (MEC 2017_134, NL61507.018.17) on the 2nd of October 2017. Approval of a local ethical committee and/or the Board of Directors will be obtained in each participating hospital. At the time of submission of this study protocol, the following hospitals received approval for participation and are therefore open for inclusion: Amsterdam UMC (Amsterdam), Catharina Hospital (Eindhoven), Flevo Hospital (Almere), OLVG (Amsterdam), Radboud University Medical Centre (Nijmegen) and University Medical Centre Utrecht (Utrecht). Written informed consent will be obtained from all participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Adjuvant hyperthermic intraperitoneal chemotherapy in patients with locally advanced colon cancer (COLOPEC): a multicentre, open-label, randomised trial.Lancet Gastroenterol Hepatol. 2019 Oct;4(10):761-770. doi: 10.1016/S2468-1253(19)30239-0. Epub 2019 Jul 29. Lancet Gastroenterol Hepatol. 2019. PMID: 31371228 Clinical Trial.
-
Risk of metachronous peritoneal metastases in patients with pT4a versus pT4b colon cancer: An international multicentre cohort study.Eur J Surg Oncol. 2021 Sep;47(9):2405-2413. doi: 10.1016/j.ejso.2021.05.009. Epub 2021 May 15. Eur J Surg Oncol. 2021. PMID: 34030920
-
Patients with extensive regional lymph node involvement (pN2) following potentially curative surgery for colorectal cancer are at increased risk for developing peritoneal metastases: a retrospective single-institution study.Colorectal Dis. 2019 Mar;21(3):287-296. doi: 10.1111/codi.14481. Epub 2018 Dec 21. Colorectal Dis. 2019. PMID: 30457185
-
Pretherapeutic evaluation of patients with upper gastrointestinal tract cancer using endoscopic and laparoscopic ultrasonography.Dan Med J. 2012 Dec;59(12):B4568. Dan Med J. 2012. PMID: 23290296 Review.
-
The radiologist's role in the multidisciplinary team for patients with colon cancer peritoneal metastases.Surg Oncol. 2022 Mar;40:101690. doi: 10.1016/j.suronc.2021.101690. Epub 2021 Nov 24. Surg Oncol. 2022. PMID: 34839197 Review.
Cited by
-
A Prediction Model Intended for Exploratory Laparoscopy Risk Stratification in Colorectal Cancer Patients With Potential Occult Peritoneal Metastasis.Front Oncol. 2022 Jul 13;12:943951. doi: 10.3389/fonc.2022.943951. eCollection 2022. Front Oncol. 2022. PMID: 35912189 Free PMC article.
-
A Prediction Model for Metachronous Peritoneal Carcinomatosis in Patients with Stage T4 Colon Cancer after Curative Resection.Cancers (Basel). 2021 Jun 4;13(11):2808. doi: 10.3390/cancers13112808. Cancers (Basel). 2021. PMID: 34200032 Free PMC article.
-
Early postoperative outcomes of staging laparoscopy for peritoneal metastases with or without pressurized intra-peritoneal aerosol chemotherapy (PIPAC).BMC Surg. 2022 Mar 30;22(1):122. doi: 10.1186/s12893-022-01572-5. BMC Surg. 2022. PMID: 35354404 Free PMC article.
-
Watchful waiting for small non-functional pancreatic neuroendocrine tumours: nationwide prospective cohort study (PANDORA).Br J Surg. 2021 Aug 19;108(8):888-891. doi: 10.1093/bjs/znab088. Br J Surg. 2021. PMID: 33783475 Free PMC article.
-
Epidemiology, oncologic results and risk stratification model for metachronous peritoneal metastases after surgery for pT4 colon cancers: results from an observational retrospective multicentre long-term follow-up study.Tech Coloproctol. 2023 Nov;27(11):1025-1036. doi: 10.1007/s10151-023-02816-z. Epub 2023 May 30. Tech Coloproctol. 2023. PMID: 37248370
References
-
- Verwaal VJ, van Ruth S, de Bree E, van Sloothen GW, van Tinteren H, Boot H, Zoetmulder FA. Randomized trial of cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy and palliative surgery in patients with peritoneal carcinomatosis of colorectal cancer. J Clin Oncol. 2003;21:3737–3743. doi: 10.1200/JCO.2003.04.187. - DOI - PubMed
-
- Pelz JO, Chua TC, Esquivel J, Stojadinovic A, Doerfer J, Morris DL, Maeder U, Germer CT, Kerscher AG. Evaluation of best supportive care and systemic chemotherapy as treatment stratified according to the retrospective peritoneal surface disease severity score (PSDSS) for peritoneal carcinomatosis of colorectal origin. BMC Cancer. 2010;10:689. doi: 10.1186/1471-2407-10-689. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
