

Polytherapy and Targeted Cancer Drug Resistance
- PMID: 30898264
- PMCID: PMC6446041
- DOI: 10.1016/j.trecan.2019.02.003
Polytherapy and Targeted Cancer Drug Resistance
Abstract
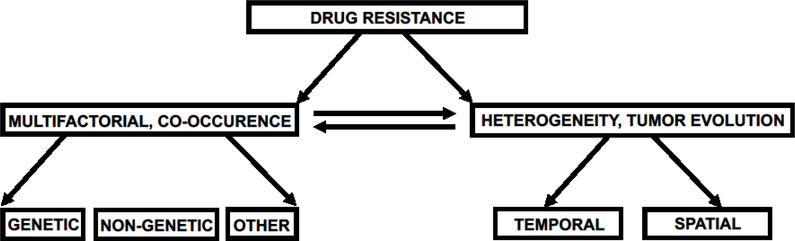
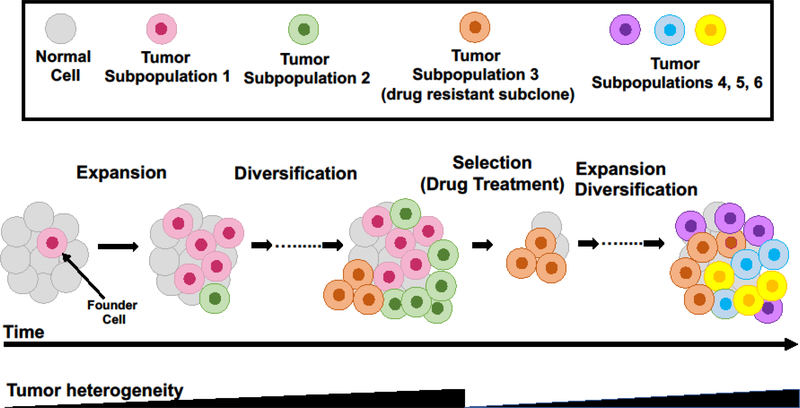
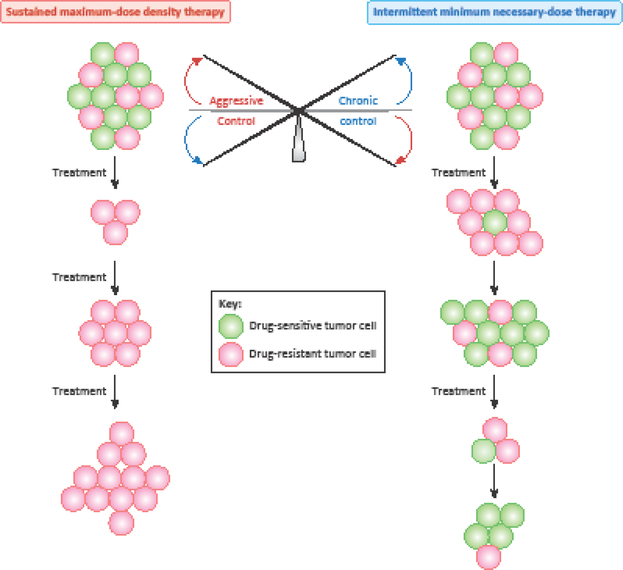
A current challenge in cancer treatment is drug resistance. Even the most effective therapies often fail to produce a complete and durable tumor response and ultimately give rise to therapy resistance and tumor relapse. However, how resistance arises in cancer remains incompletely understood. While drug resistance in cancer is thought to be driven by irreversible genetic mutations, emerging evidence also implicates reversible proteomic and epigenetic mechanisms in the development of drug resistance. Tumor microenvironment-mediated mechanisms and tumor heterogeneity can significantly contribute to cancer treatment resistance. Here, we discuss the diverse and dynamic strategies that cancers use to evade drug response, the promise of upfront combination and intermittent therapies and therapy switching in forestalling resistance, and epigenetic reprogramming to combat resistance.
Keywords: cancer evolution; drug resistance; epigenetics; genetics; molecular targets; polytherapy; targeted therapy.
Copyright © 2019 Elsevier Inc. All rights reserved.
Conflict of interest statement
Potential Conflicts of Interest.
N.C. declares no competing interests.
Figures
References
-
- Nikolaou M et al. (2018) The challenge of drug resistance in cancer treatment: a current overview. Clin Exp Metastasis 35 (4), 309–318. - PubMed
-
- Gottesman MM et al. (2016) Toward a Better Understanding of the Complexity of Cancer Drug Resistance. Annu Rev Pharmacol Toxicol 56, 85–102. - PubMed
-
- Garraway LA and Janne PA (2012) Circumventing cancer drug resistance in the era of personalized medicine. Cancer Discov 2 (3), 214–26. - PubMed
-
- Lee HJ et al. (2014) Drug resistance via feedback activation of Stat3 in oncogene-addicted cancer cells. Cancer Cell 26 (2), 207–21. - PubMed
