

Retrospective study of irrational prescribing in French paediatric hospital: prevalence of inappropriate prescription detected by Pediatrics: Omission of Prescription and Inappropriate prescription (POPI) in the emergency unit and in the ambulatory setting
- PMID: 30898791
- PMCID: PMC6475152
- DOI: 10.1136/bmjopen-2017-019186
Retrospective study of irrational prescribing in French paediatric hospital: prevalence of inappropriate prescription detected by Pediatrics: Omission of Prescription and Inappropriate prescription (POPI) in the emergency unit and in the ambulatory setting
Abstract
Background and objective: Pediatrics: Omission of Prescription and Inappropriate prescription (POPI) is the first detection tool for potentially inappropriate medicines (PIMs) and potentially prescribing omissions (PPOs) in paediatrics. The aim of this study was to evaluate the prevalence of PIM and PPO detected by POPI regarding prescriptions in hospital and for outpatients. The second objective is to determine the risk factors related to PIM and PPO.
Design: A retrospective, descriptive study was conducted in the emergency department (ED) and community pharmacy (CP) during 6 months. POPI was used to identify PIM and PPO.
Setting: Robert-Debré Hospital (France) and Albaret community pharmacy (Seine and Marne).
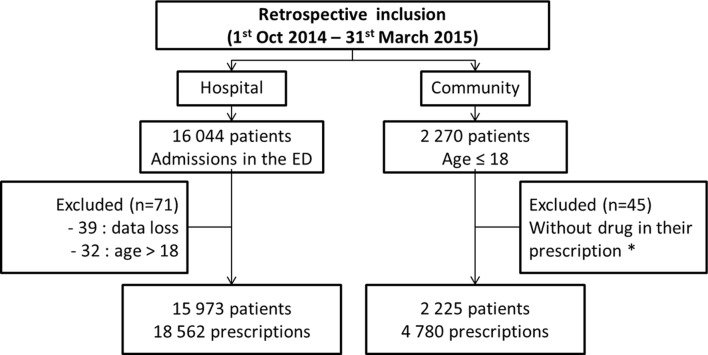
Participants: Patients who were under 18 years old and who had one or more drugs prescribed were included. Exclusion criteria consisted of inaccessible medical records for patients consulted in ED and prescription without drugs for outpatients.
Primary and secondary outcome measures: PIM and PPO rate and risk factors.
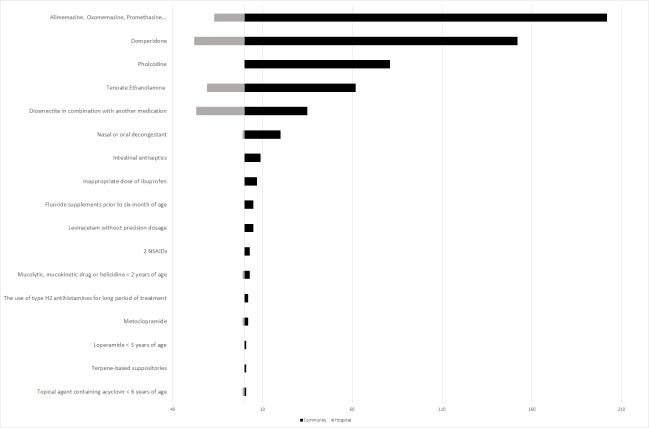
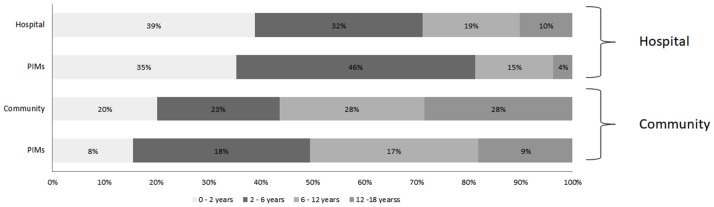
Results: At the ED, 18 562 prescriptions of 15 973 patients and 4780 prescriptions of 2225 patients at the CP were analysed. The PIM rate and PPO rate were, respectively, 2.9% and 2.3% at the ED and 12.3% and 6.1% at the CP. Respiratory and digestive diseases had the highest rate of PIM.
Conclusion: This is the first study to assess the prevalence of PIM and PPO detected by POPI in a paediatric population. This study assessed PIMs or PPOs within a hospital and a community pharmacy. POPI could be used to improve drug use and patient care and to limit hospitalisation and adverse drug reaction. A prospective multicentric study should be conducted to evaluate the impact and benefit of implementing POPI in clinical practice.
Keywords: detection; inappropriate prescription; omission; tool.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Bates DW, Cullen DJ, Laird N, et al. Incidence of adverse drug events and potential adverse drug events. Implications for prevention. ADE Prevention Study Group. JAMA 1995;274:29–34. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous