

Transmission patterns of HIV-1 non-R5 strains in Poland
- PMID: 30899060
- PMCID: PMC6428829
- DOI: 10.1038/s41598-019-41407-7
Transmission patterns of HIV-1 non-R5 strains in Poland
Abstract
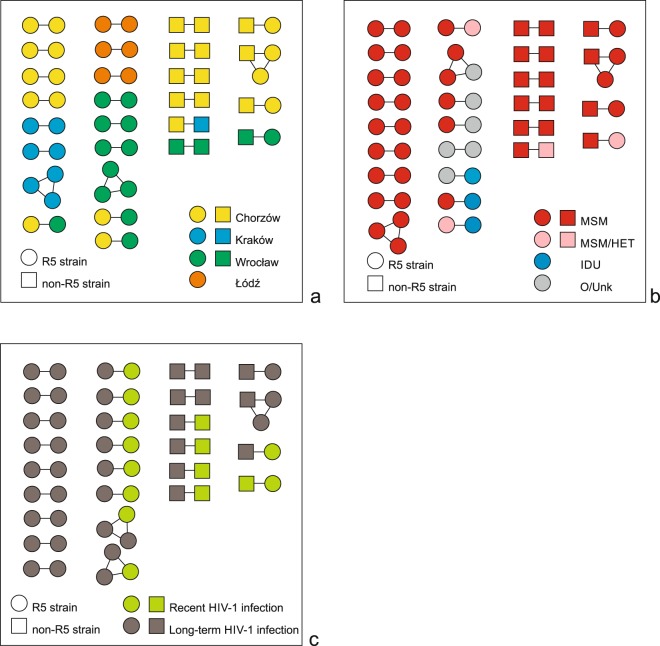
HIV-1 env sequencing enables predictions of viral coreceptor tropism and phylogenetic investigations of transmission events. The aim of the study was to estimate the contribution of non-R5 strains to the viral spread in Poland. Partial proviral env sequences were retrieved from baseline blood samples of patients with newly diagnosed HIV-1 infection between 2008-2014, including 46 patients with recent HIV-1 infection (RHI), and 246 individuals with long-term infection (LTHI). These sequences were subjected to the genotypic coreceptor tropism predictions and phylogenetic analyses to identify transmission clusters. Overall, 27 clusters with 57 sequences (19.5%) were detected, including 15 sequences (26.3%) from patients with RHI. The proportion of non-R5 strains among all study participants was 23.3% (68/292), and was comparable between patients with RHI and LTHI (11/46, 23.9% vs 57/246, 23.2%; p = 1.000). All 11 patients with non-R5 strains and RHI were men having sex with men (MSM). Among these patients, 4 had viral sequences grouped within phylogenetic cluster with another sequence of non-R5 strain obtained from patient with LTHI, indicating potential acquisition of non-R5 HIV-1 for at least 4/46 (8.7%) patients with RHI. We were unable to confirm the contribution of patients with RHI to the forward transmission of non-R5 strains, but a relatively high proportion of non-R5 strains among them deserves attention due to the limited susceptibility to CCR5 antagonists.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Raymond S, et al. CXCR4-using viruses in plasma and peripheral blood mononuclear cells during primary HIV-1 infection and impact on disease progression. AIDS. 2010;24:2305–2312. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
