

Ipsilesional Mu Rhythm Desynchronization and Changes in Motor Behavior Following Post Stroke BCI Intervention for Motor Rehabilitation
- PMID: 30899211
- PMCID: PMC6417367
- DOI: 10.3389/fnins.2019.00053
Ipsilesional Mu Rhythm Desynchronization and Changes in Motor Behavior Following Post Stroke BCI Intervention for Motor Rehabilitation
Abstract
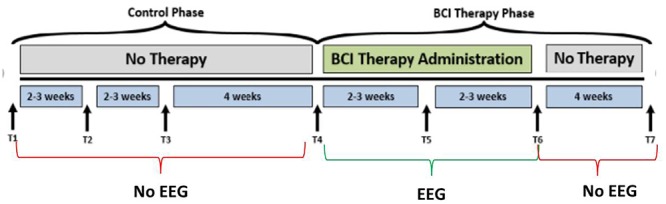
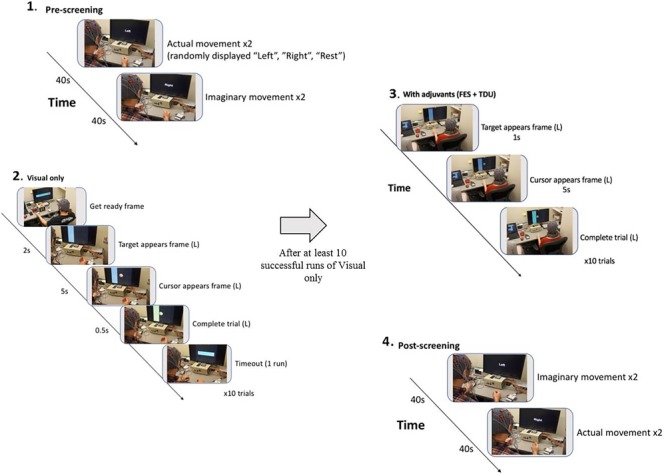
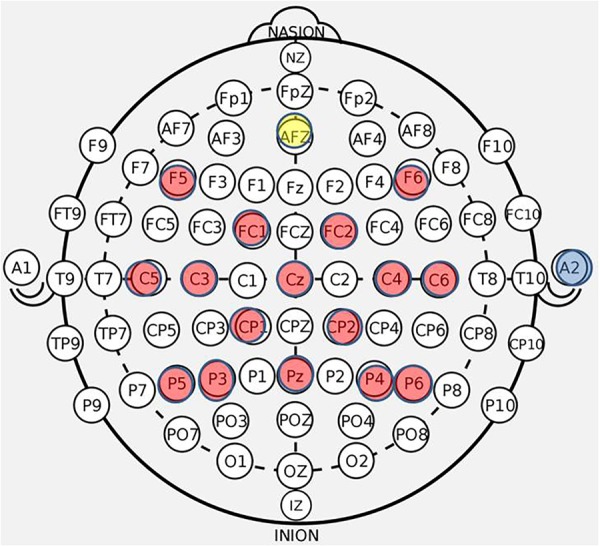
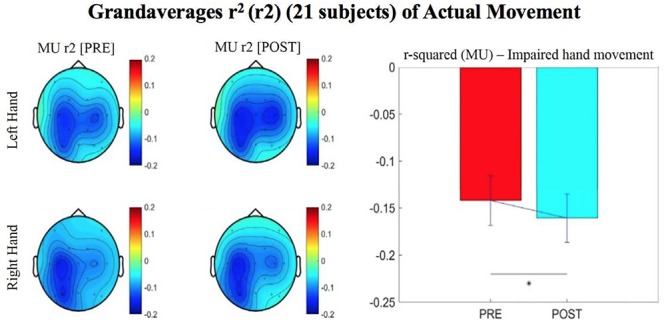
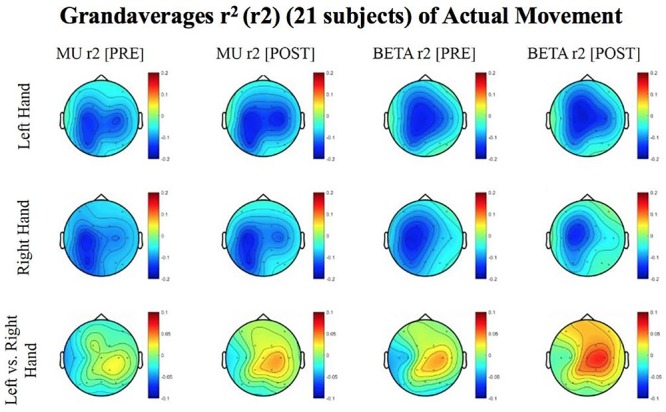
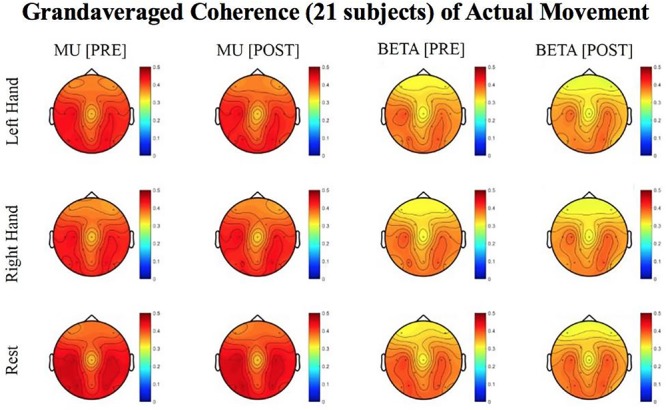
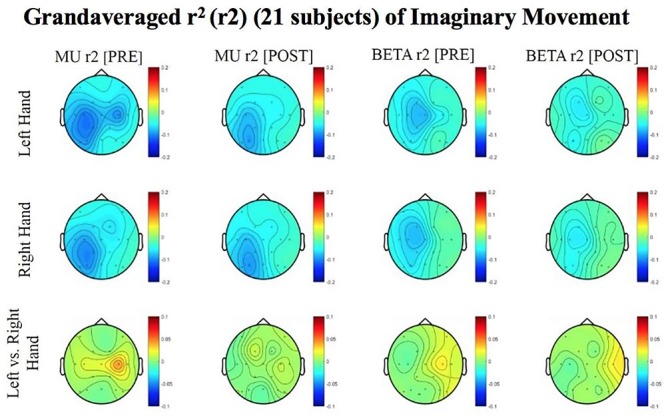
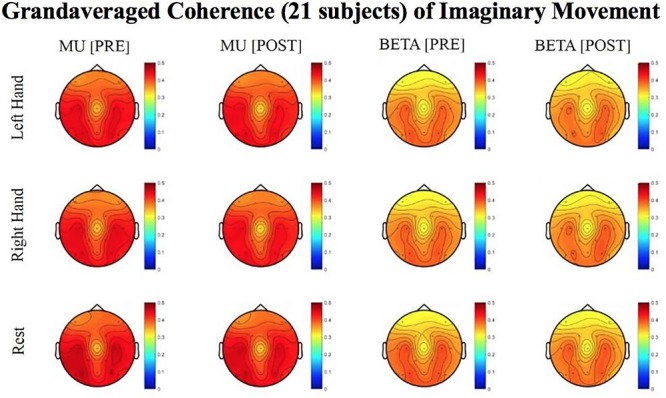
Loss of motor function is a common deficit following stroke insult and often manifests as persistent upper extremity (UE) disability which can affect a survivor's ability to participate in activities of daily living. Recent research suggests the use of brain-computer interface (BCI) devices might improve UE function in stroke survivors at various times since stroke. This randomized crossover-controlled trial examines whether intervention with this BCI device design attenuates the effects of hemiparesis, encourages reorganization of motor related brain signals (EEG measured sensorimotor rhythm desynchronization), and improves movement, as measured by the Action Research Arm Test (ARAT). A sample of 21 stroke survivors, presenting with varied times since stroke and levels of UE impairment, received a maximum of 18-30 h of intervention with a novel electroencephalogram-based BCI-driven functional electrical stimulator (EEG-BCI-FES) device. Driven by spectral power recordings from contralateral EEG electrodes during cued attempted grasping of the hand, the user's input to the EEG-BCI-FES device modulates horizontal movement of a virtual cursor and also facilitates concurrent stimulation of the impaired UE. Outcome measures of function and capacity were assessed at baseline, mid-therapy, and at completion of therapy while EEG was recorded only during intervention sessions. A significant increase in r-squared values [reflecting Mu rhythm (8-12 Hz) desynchronization as the result of attempted movements of the impaired hand] presented post-therapy compared to baseline. These findings suggest that intervention corresponds with greater desynchronization of Mu rhythm in the ipsilesional hemisphere during attempted movements of the impaired hand and this change is related to changes in behavior as a result of the intervention. BCI intervention may be an effective way of addressing the recovery of a stroke impaired UE and studying neuromechanical coupling with motor outputs. Clinical Trial Registration: ClinicalTrials.gov, identifier NCT02098265.
Keywords: brain–computer interface;; hemiparesis; r-squared; coherence; chronic; acute; neuroplasticity; homunculus.
Figures
Similar articles
-
Ipsilesional Mu Rhythm Desynchronization Correlates With Improvements in Affected Hand Grip Strength and Functional Connectivity in Sensorimotor Cortices Following BCI-FES Intervention for Upper Extremity in Stroke Survivors.Front Hum Neurosci. 2021 Oct 28;15:725645. doi: 10.3389/fnhum.2021.725645. eCollection 2021. Front Hum Neurosci. 2021. PMID: 34776902 Free PMC article.
-
Behavioral Outcomes Following Brain-Computer Interface Intervention for Upper Extremity Rehabilitation in Stroke: A Randomized Controlled Trial.Front Neurosci. 2018 Nov 8;12:752. doi: 10.3389/fnins.2018.00752. eCollection 2018. Front Neurosci. 2018. PMID: 30467461 Free PMC article.
-
Sensorimotor Rhythm-Brain Computer Interface With Audio-Cue, Motor Observation and Multisensory Feedback for Upper-Limb Stroke Rehabilitation: A Controlled Study.Front Neurosci. 2022 Mar 11;16:808830. doi: 10.3389/fnins.2022.808830. eCollection 2022. Front Neurosci. 2022. PMID: 35360158 Free PMC article.
-
Immediate and long-term effects of BCI-based rehabilitation of the upper extremity after stroke: a systematic review and meta-analysis.J Neuroeng Rehabil. 2020 Apr 25;17(1):57. doi: 10.1186/s12984-020-00686-2. J Neuroeng Rehabil. 2020. PMID: 32334608 Free PMC article.
-
Brain-computer interfaces for post-stroke motor rehabilitation: a meta-analysis.Ann Clin Transl Neurol. 2018 Mar 25;5(5):651-663. doi: 10.1002/acn3.544. eCollection 2018 May. Ann Clin Transl Neurol. 2018. PMID: 29761128 Free PMC article. Review.
Cited by
-
BCI-FES With Multimodal Feedback for Motor Recovery Poststroke.Front Hum Neurosci. 2022 Jul 6;16:725715. doi: 10.3389/fnhum.2022.725715. eCollection 2022. Front Hum Neurosci. 2022. PMID: 35874158 Free PMC article.
-
An Evaluation Model for Brain Ischemia Protection in Mice by Low-Intensity Pulsed Ultrasound Stimulation Based on Functional Cortico-Muscular Coupling.Bioengineering (Basel). 2025 May 17;12(5):541. doi: 10.3390/bioengineering12050541. Bioengineering (Basel). 2025. PMID: 40428160 Free PMC article.
-
Clinical applications of neurofeedback based on sensorimotor rhythm: a systematic review and meta-analysis.Front Neurosci. 2023 Nov 20;17:1195066. doi: 10.3389/fnins.2023.1195066. eCollection 2023. Front Neurosci. 2023. PMID: 38053609 Free PMC article.
-
Brain Connectivity Changes During Bimanual and Rotated Motor Imagery.IEEE J Transl Eng Health Med. 2022 Apr 14;10:2100408. doi: 10.1109/JTEHM.2022.3167552. eCollection 2022. IEEE J Transl Eng Health Med. 2022. PMID: 35492507 Free PMC article.
-
Brain-Computer Interface Training With Functional Electrical Stimulation: Facilitating Changes in Interhemispheric Functional Connectivity and Motor Outcomes Post-stroke.Front Neurosci. 2021 Sep 27;15:670953. doi: 10.3389/fnins.2021.670953. eCollection 2021. Front Neurosci. 2021. PMID: 34646112 Free PMC article.
References
-
- Ang K., Guan C. (2013). Brain-computer interface in stroke rehabilitation. J. Comput. Sci. Eng. 7 139–146. 10.5626/JCSE.2013.7.2.139 - DOI
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous