

Anatomic Reconstruction of the Posterolateral Corner: An All-Arthroscopic Technique
- PMID: 30899667
- PMCID: PMC6410677
- DOI: 10.1016/j.eats.2018.10.010
Anatomic Reconstruction of the Posterolateral Corner: An All-Arthroscopic Technique
Abstract
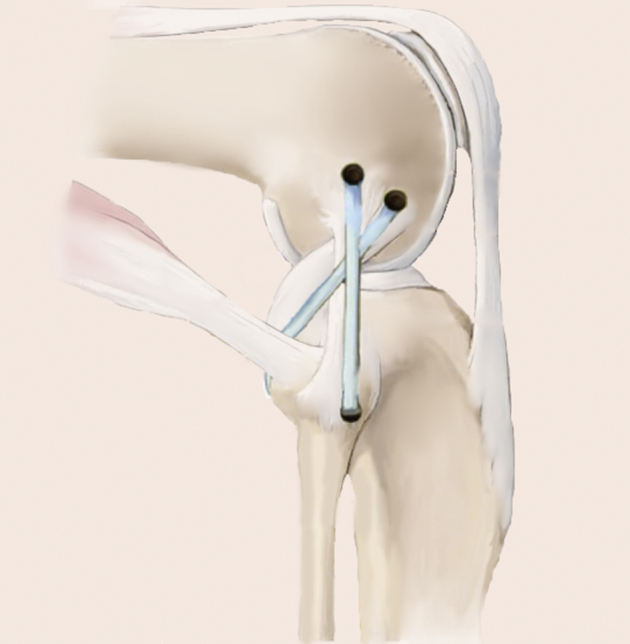
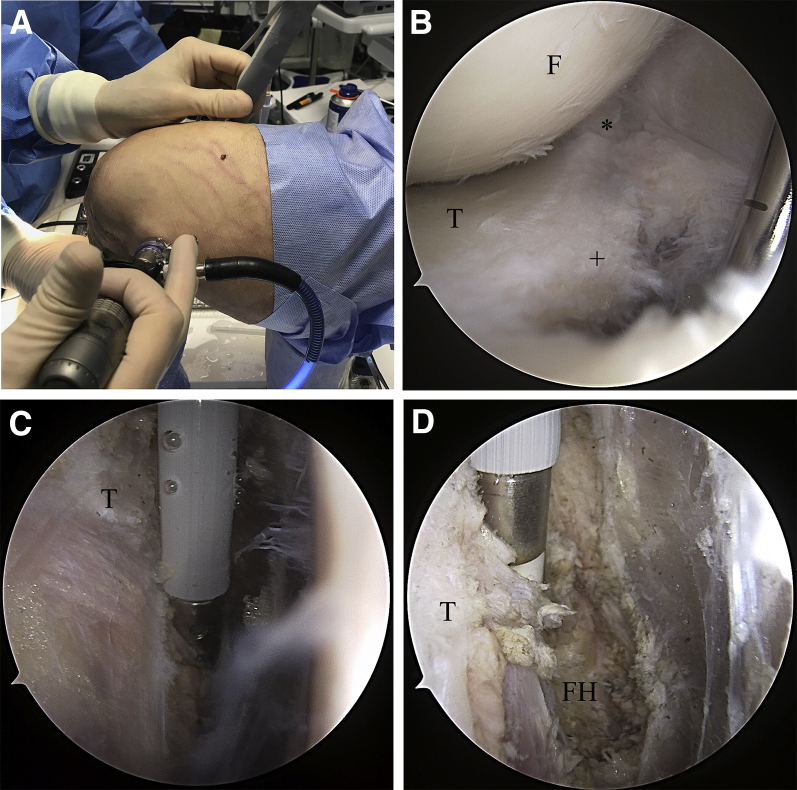
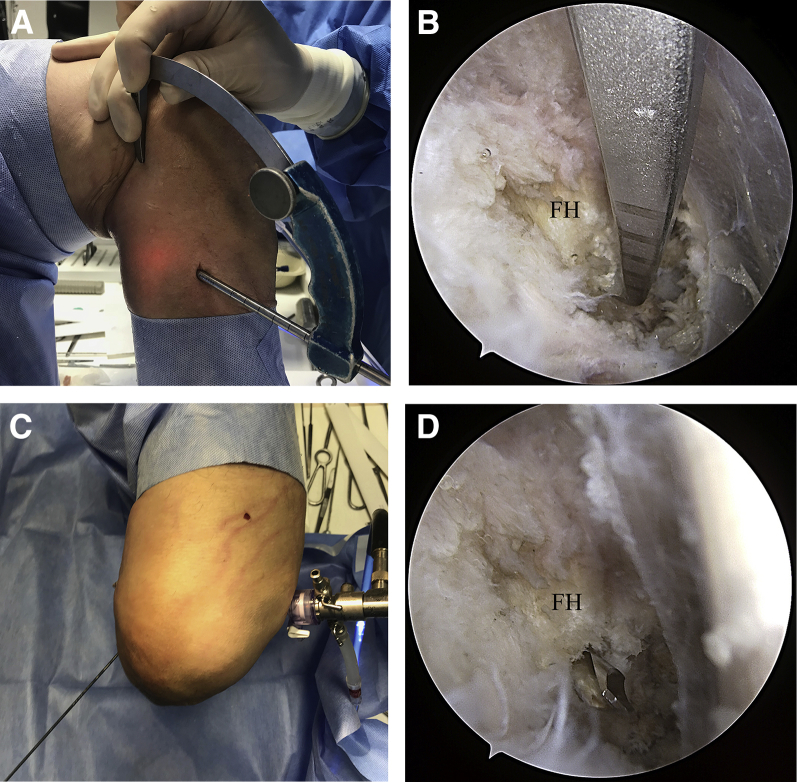
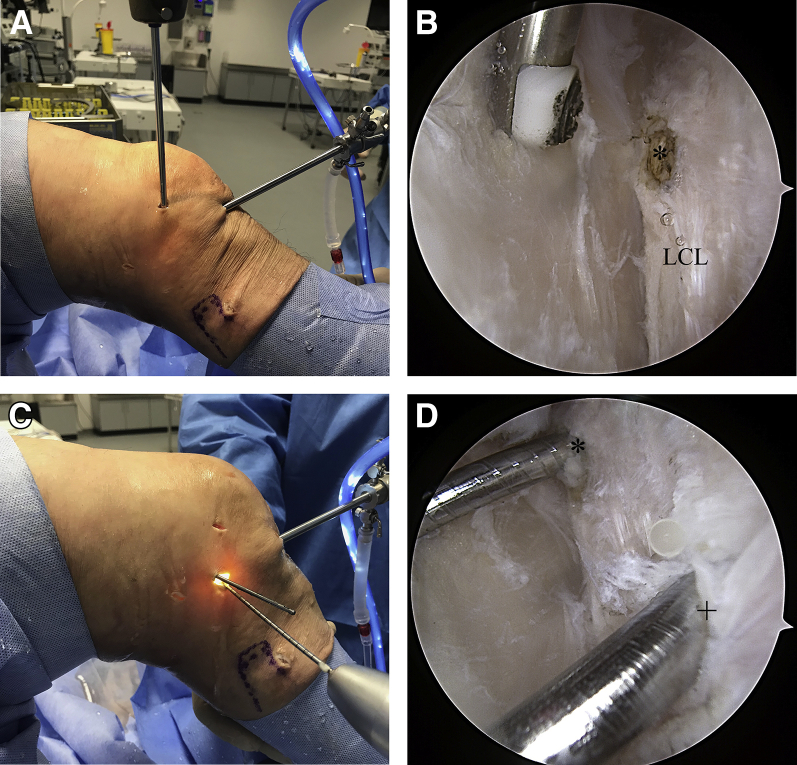
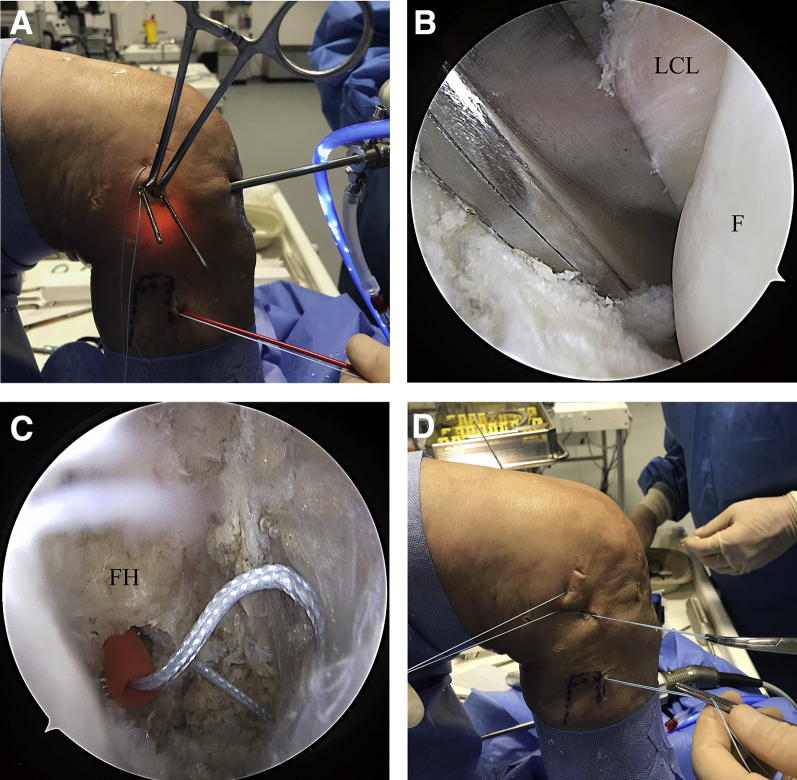
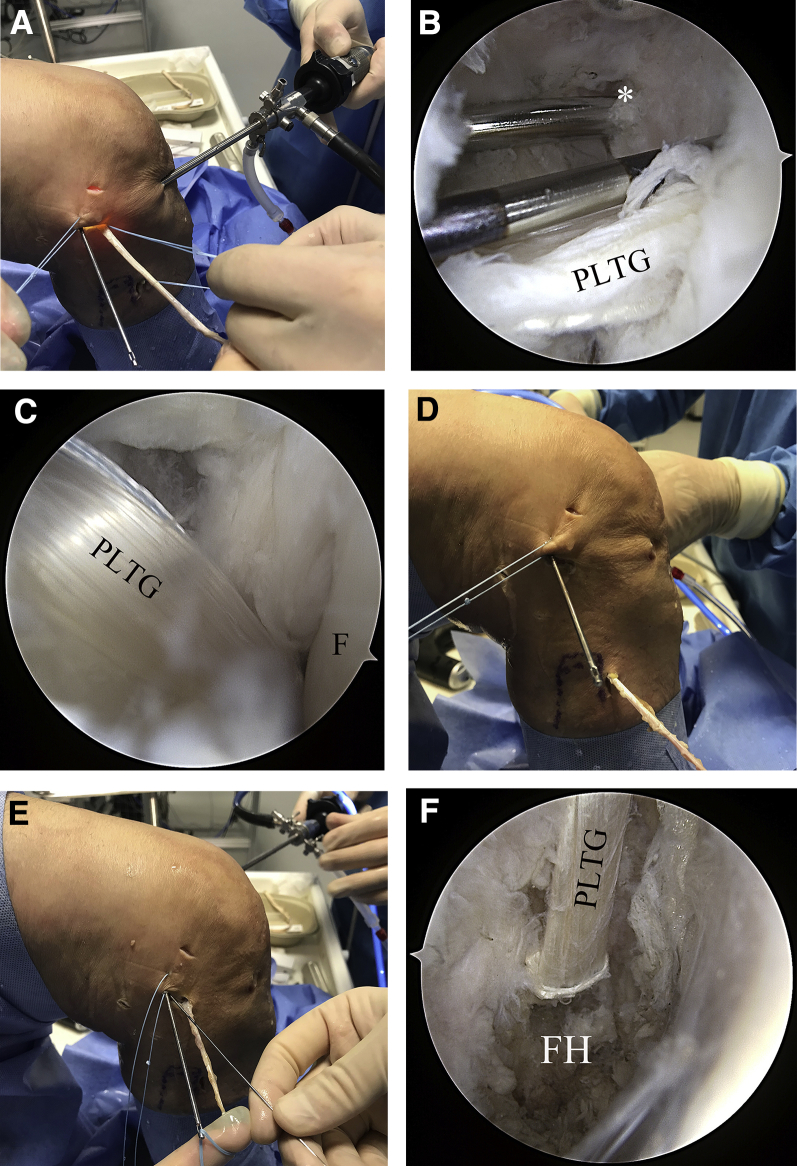
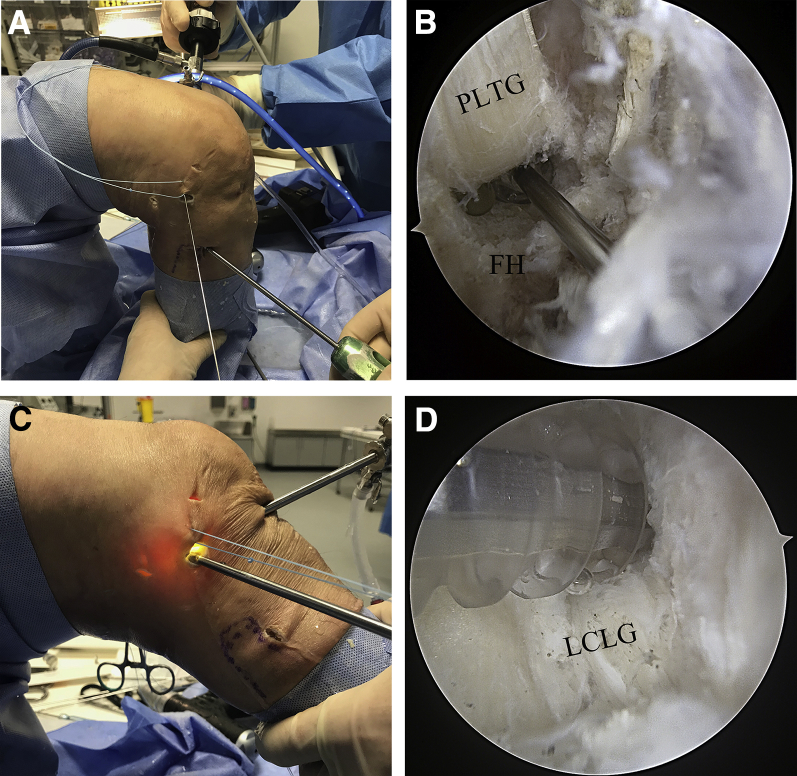
Injuries of the posterolateral corner (PLC) of the knee lead to chronic lateral and external rotational instability. Successful treatment of PLC injuries requires an understanding of the complex anatomy and biomechanics of the PLC. Several open PLC reconstruction techniques have been published. It is understood that anatomic reconstruction is superior to extra-anatomic techniques, leading to better clinical results. An open, anatomic, fibula-based technique for reconstruction to address lateral and rotational instability has been described. However, when an open technique is used, surgeon and patient are faced with disadvantages, such as soft tissue damage or exposure of vulnerable structures. Few arthroscopic techniques for tibia- or fibula-based reconstruction of rotational posterolateral instability have been described. A complete arthroscopic stabilization of the combined lateral and posterolateral rotational instability of the knee has not yet been described. We therefore present the first all-arthroscopic technique for complete PLC reconstruction, based on an open technique described previously. All relevant landmarks of the PLC can be arthroscopically visualized in detail, allowing safe and effective treatment of PLC injuries.
Figures
References
-
- LaPrade R.F., Griffith C.J., Coobs B.R., Geeslin A.G., Johansen S., Engebretsen L. Improving outcomes for posterolateral knee injuries. J Orthop Res. 2014;32:485–491. - PubMed
-
- Frosch K.-H., Akoto R., Heitmann M., Enderle E., Giannakos A., Preiss A. Arthroscopic reconstruction of the popliteus complex: Accuracy and reproducibility of a new surgical technique. Knee Surg Sports Traumatol Arthrosc. 2015;23:3114–3120. - PubMed
-
- Thaunat M., Pioger C., Chatellard R., Conteduca J., Khaleel A., Sonnery-Cottet B. The arcuate ligament revisited: Role of the posterolateral structures in providing static stability in the knee joint. Knee Surg Sports Traumatol Arthrosc. 2014;22:2121–2127. - PubMed
-
- Domnick C., Frosch K.H., Raschke M.J. Kinematics of different components of the posterolateral corner of the knee in the lateral collateral ligament-intact state: A human cadaveric study. Arthroscopy. 2017;33:1821–1830. - PubMed
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
