

Acanthamoeba keratitis - Clinical signs, differential diagnosis and treatment
- PMID: 30899841
- PMCID: PMC6407156
- DOI: 10.1016/j.joco.2018.09.008
Acanthamoeba keratitis - Clinical signs, differential diagnosis and treatment
Abstract
Purpose: To summarize actual literature data on clinical signs, differential diagnosis, and treatment of acanthamoeba keratitis.
Methods: Review of literature.
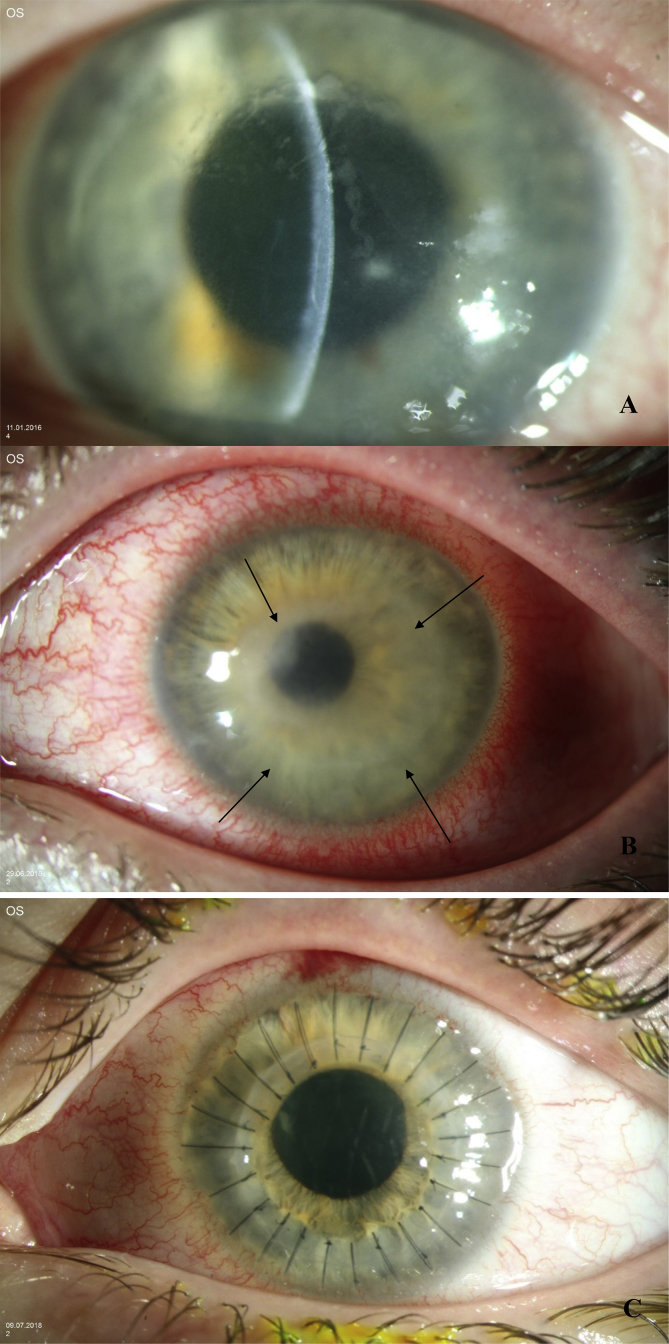
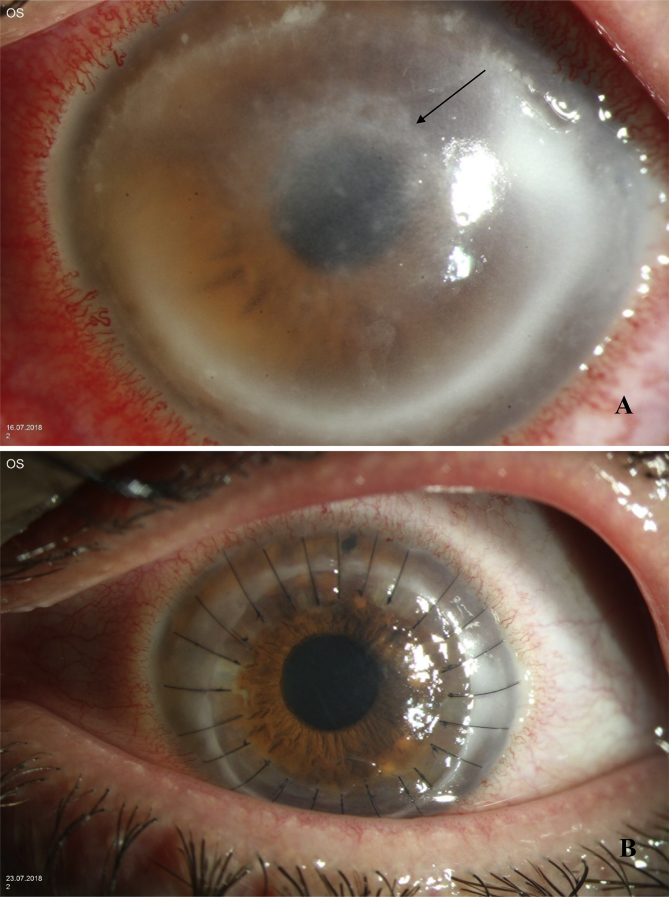
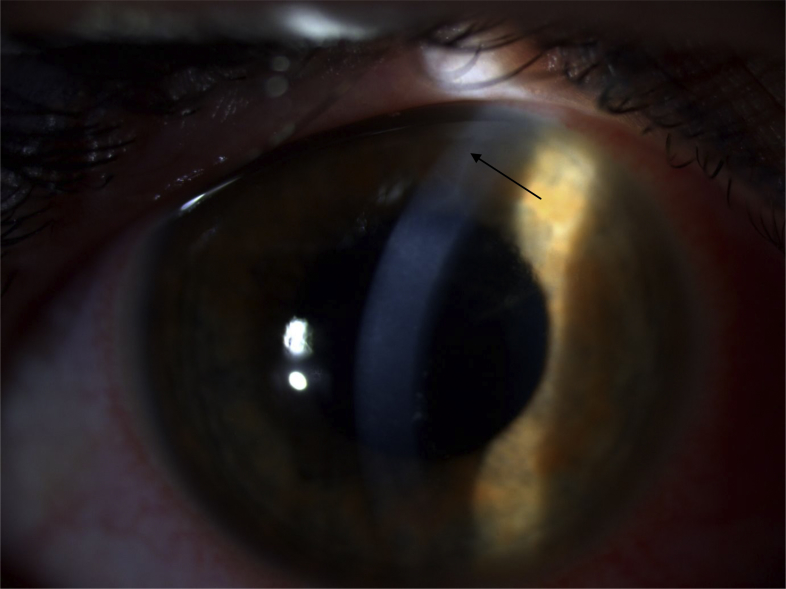
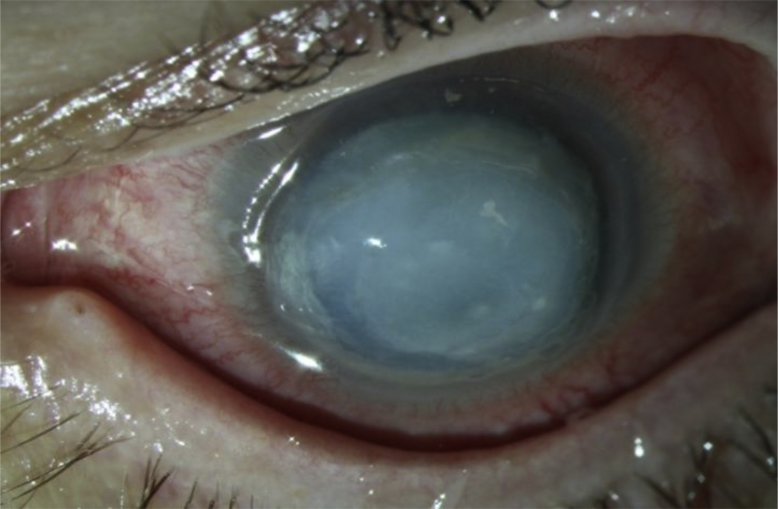
Results: Clinical signs of acanthamoeba keratitis are in early stages grey-dirty epithelium, pseudodendritiformic epitheliopathy, perineuritis, multifocal stromal infiltrates, ring infiltrate and in later stages scleritis, iris atrophy, anterior synechiae, secondary glaucoma, mature cataract, and chorioretinitis. As conservative treatment, we use up to one year triple-topical therapy (polyhexamethylene-biguanide, propamidine-isethionate, neomycin). In therapy resistant cases, surgical treatment options such as corneal cryotherapy, amniotic membrane transplantation, riboflavin-UVA cross-linking, and penetrating keratoplasty are applied.
Conclusion: With early diagnosis and conservative or surgical treatment, acanthamoeba keratitis heals in most cases.
Keywords: Acanthamoeba; Contact lens; Cornea; Keratitis.
Figures
References
-
- Meltendorf C., Duncker G. Acanthamoeba keratitis. Klin Monatsbl Augenheilkd. 2011;228(3):R29–R43. [Article in German] - PubMed
-
- Szentmáry N., Göbels S., Matoula P., Schirra F., Seitz B. Acanthamoeba keratitis – a rare and often late diagnosed disease. Klin Monbl Augenheilkd. 2012;229(5):521–528. [Article in German] - PubMed
-
- Gupta S., Das S.R. Stock cultures of free-living amebas: effct of temperature on viability and pathogenicity. J Parasitol. 1999;85(1):137–139. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
