

Paying for Hemodialysis in Kerala, India: A Description of Household Financial Hardship in the Context of Medical Subsidy
- PMID: 30899866
- PMCID: PMC6409432
- DOI: 10.1016/j.ekir.2018.12.007
Paying for Hemodialysis in Kerala, India: A Description of Household Financial Hardship in the Context of Medical Subsidy
Abstract
Introduction: Many low- and middle-income countries are implementing strategies to increase dialysis availability as growing numbers of people reach end-stage renal disease. Despite efforts to subsidize care, the economic sustainability of chronic dialysis in these settings remains uncertain. We evaluated the association of medical subsidy with household financial hardship related to hemodialysis in Kerala, India, a state with high penetrance of procedure-based subsidies for patients on dialysis.
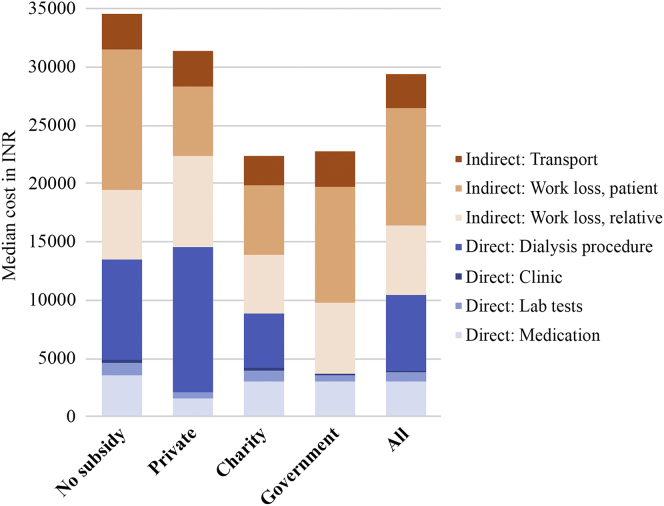
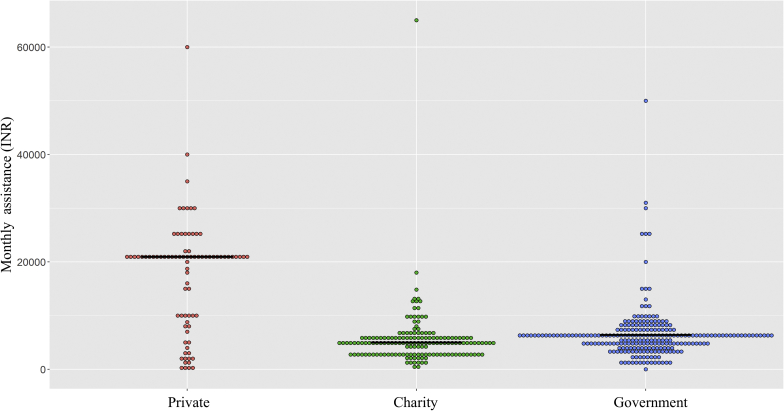
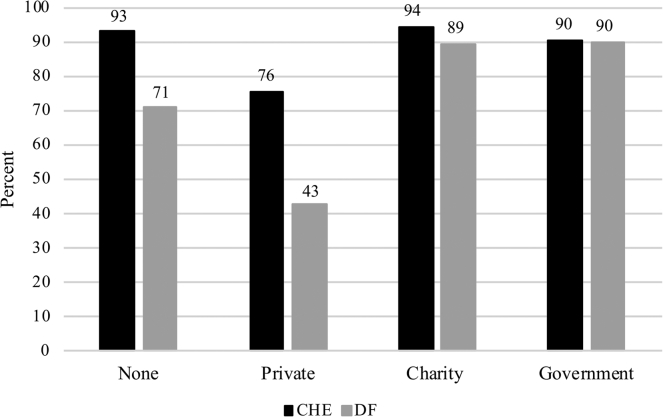
Methods: Patients on maintenance hemodialysis at 15 facilities in Kerala were administered a questionnaire that ascertained demographics, dialysis details, and household finances. We estimated direct and indirect costs of hemodialysis, and described the use of medical subsidy. We evaluated whether presence of subsidy (private, charity, or government-sponsored) was associated with lower catastrophic health expenditure (defined as ≥40% of nonsubsistence expenditure spent on dialysis) or distress financing.
Results: Of the 835 patients surveyed, 759 (91%) reported their households experienced catastrophic health expenditure, and 644 (77%) engaged in distress financing. Median dialysis-related expenditure was 80% (25th-75th percentile: 60%-90%) of household nonsubsistence expenditure. Government subsidies were used by 238 (29%) of households, 139 (58%) of which were in the lowest income category. Catastrophic health expenditure was present in 215 (90%) of households receiving government subsidy and 332 (93%) without subsidy.
Conclusions: Provision of medical subsidy in Kerala, India was not associated with lower rates of household financial hardship related to long-term hemodialysis therapy. Transparent counseling on impending costs and innovative strategies to mitigate household financial distress are necessary for persons with end-stage renal disease in resource-limited settings.
Keywords: chronic kidney disease; health financing; hemodialysis.
Figures
Comment in
-
Financial toxicity and dialysis: Autonomy and truth-telling in resource-limited settings.Indian J Med Ethics. 2023 Jan-Mar;VIII(1):46-52. doi: 10.20529/IJME.2022.067. Epub 2022 Sep 3. Indian J Med Ethics. 2023. PMID: 36420603
References
-
- Morad Z., Choong H.L., Tungsanga K. Funding renal replacement therapy in southeast Asia: building public-private partnerships in Singapore, Malaysia, Thailand, and Indonesia. Am J Kidney Dis. 2015;65:799–805. - PubMed
-
- Tantivess S., Werayingyong P., Chuengsaman P. Universal coverage of renal dialysis in Thailand: promise, progress, and prospects. BMJ. 2013;346:f462. - PubMed
-
- Jha V., Martin D.E., Bargman J.M. Ethical issues in dialysis therapy. Lancet. 2017;389:1851–1856. - PubMed
-
- Garg C.C., Karan A.K. Reducing out-of-pocket expenditures to reduce poverty: a disaggregated analysis at rural-urban and state level in India. Health Policy Plan. 2009;24:116–128. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
